

Single-center real-life experience with testosterone treatment in adult men with Prader-Willi syndrome
- PMID: 35532976
- PMCID: PMC9541274
- DOI: 10.1002/ajmg.a.62770
Single-center real-life experience with testosterone treatment in adult men with Prader-Willi syndrome
Abstract
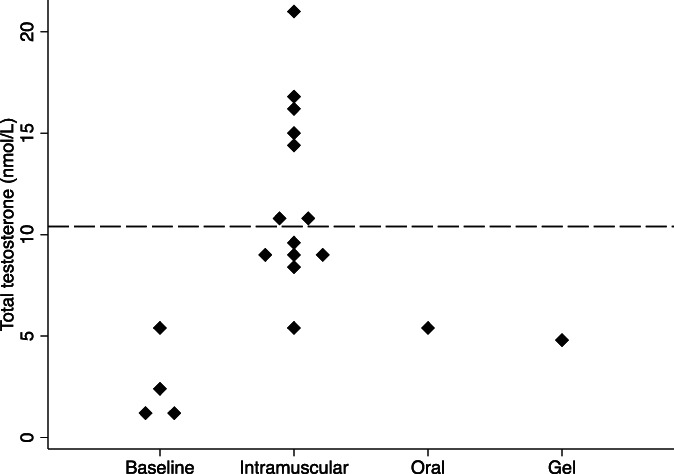
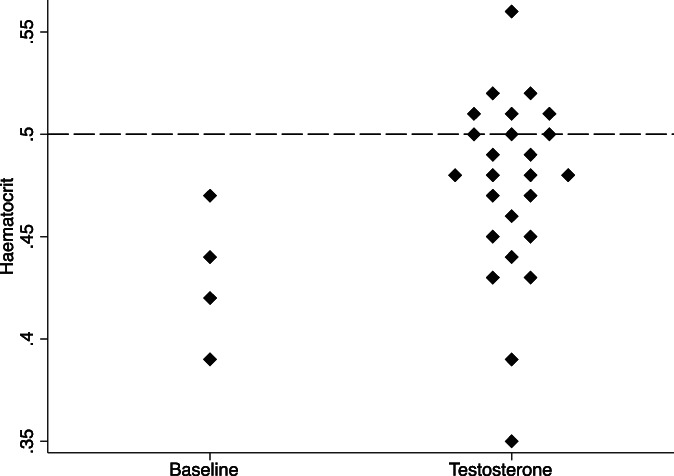
Hypogonadism is the most frequent hormonal deficiency in individuals with Prader-Willi syndrome (PWS). This often necessitates testosterone treatment, but limited data are available to guide testosterone treatment in adult men with PWS. We aimed to evaluate the serum testosterone concentrations and adverse effects of testosterone treatment in individuals with PWS attending a specialist obesity management service. A retrospective audit was undertaken at Austin Health, Melbourne between January 2010 and April 2021. Main outcome measures were testosterone formulation and dose, serum total testosterone concentration, and prevalence of polycythemia and behavioral disturbance. Data were available for eight individuals with median baseline age 19 years (range, 19-42) and BMI 37 kg/m2 (range, 27-71). Six men had obstructive sleep apnea; none were smokers. Baseline testosterone concentration was 1.8 nmol/L (IQR, 1.1-3.3) with hematocrit 0.43. Testosterone formulations were intramuscular testosterone undecanoate (TU) 1000 mg (n = 5), transdermal testosterone gel 50 mg daily (n = 1), and oral TU 80-120 mg daily (n = 2). Median total testosterone concentration was 9.7 nmol/L (IQR, 8.5-14.7). Nine of 25 (36%) hematocrit results in six patients measured >0.50 (range, 0.50-0.56). Intramuscular TU was well tolerated and was the only formulation to achieve serum total testosterone concentrations in the adult male reference range. Worsening behavioral disturbance resulted in treatment discontinuation in one individual. Our experience reinforces the need to regular monitoring of hematocrit in men with PWS treated with testosterone. However, a worsening of behavior problems was uncommon in this series.
Keywords: Prader-Willi syndrome; hypogonadism; obesity; polycythemia; testosterone.
© 2022 The Authors. American Journal of Medical Genetics Part A published by Wiley Periodicals LLC.
Conflict of interest statement
Brendan J. Nolan reports fees from iNova pharmaceuticals for lectures unrelated to the submitted work. Priya Sumithran reports fees from Novo Nordisk for participation in a lecture unrelated to the submitted work. Joseph Proietto reports being chairman of the medical advisory board for liraglutide 3 mg and has received payment for consultancy from Astra Zeneca and Eli Lilly, and lectures from iNova pharmaceuticals unrelated to the submitted work.
Figures
References
-
- Bhasin, S. , Brito, J. P. , Cunningham, G. R. , Hayes, F. J. , Hodis, H. N. , Matsumoto, A. M. , Snyder, P. J. , Swerdloff, R. S. , Wu, F. C. , & Yialamas, M. A. (2018). Testosterone therapy in men with hypogonadism: An Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology and Metabolism, 103(5), 1715–1744. 10.1210/jc.2018-00229 - DOI - PubMed
-
- Eiholzer, U. , l'Allemand, D. , Rousson, V. , Schlumpf, M. , Gasser, T. , Girard, J. , Grüters, A. , & Simoni, M. (2006). Hypothalamic and gonadal components of hypogonadism in boys with Prader‐Labhart‐Willi syndrome. The Journal of Clinical Endocrinology and Metabolism, 91(3), 892–898. 10.1210/jc.2005-0902 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
