

Assessment of fibrinolytic status in whole blood using a dielectric coagulometry microsensor
- PMID: 35533507
- PMCID: PMC10124761
- DOI: 10.1016/j.bios.2022.114299
Assessment of fibrinolytic status in whole blood using a dielectric coagulometry microsensor
Abstract
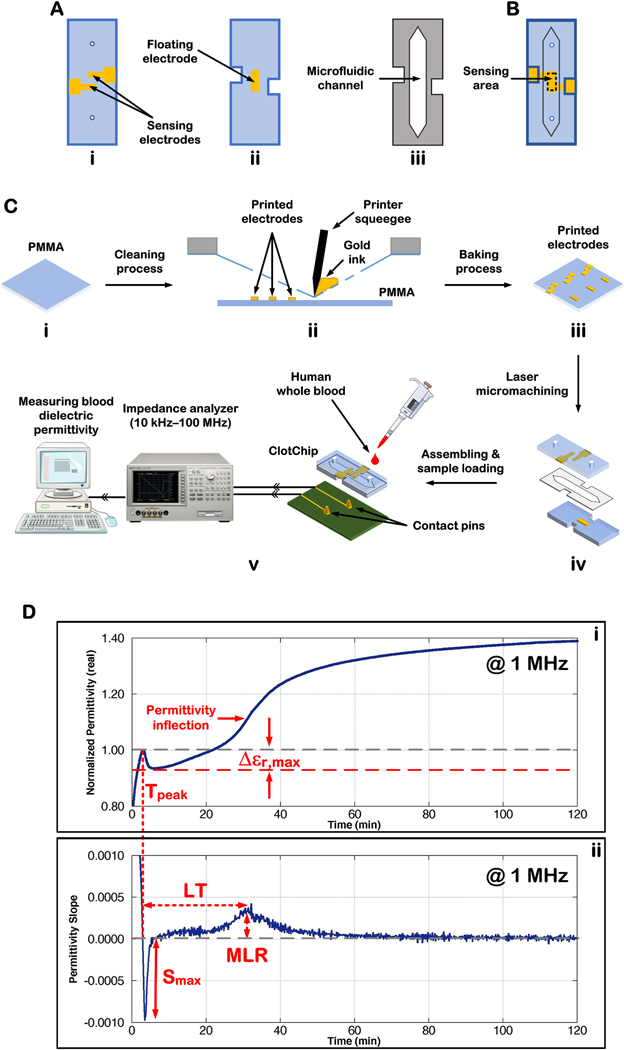
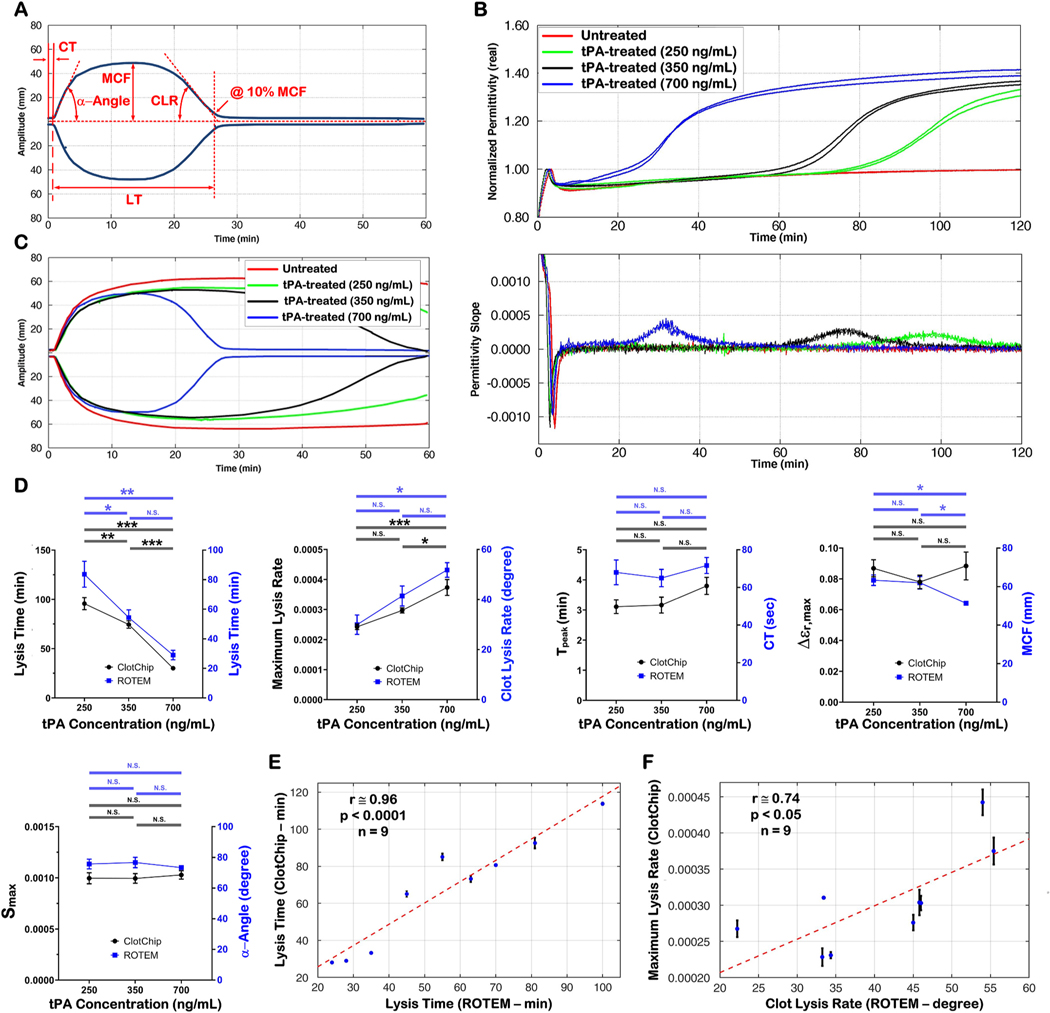
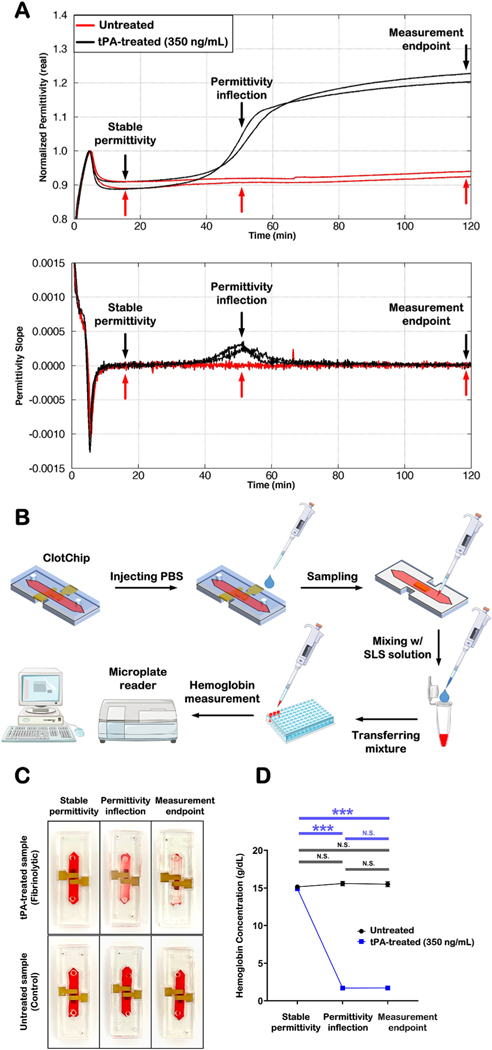
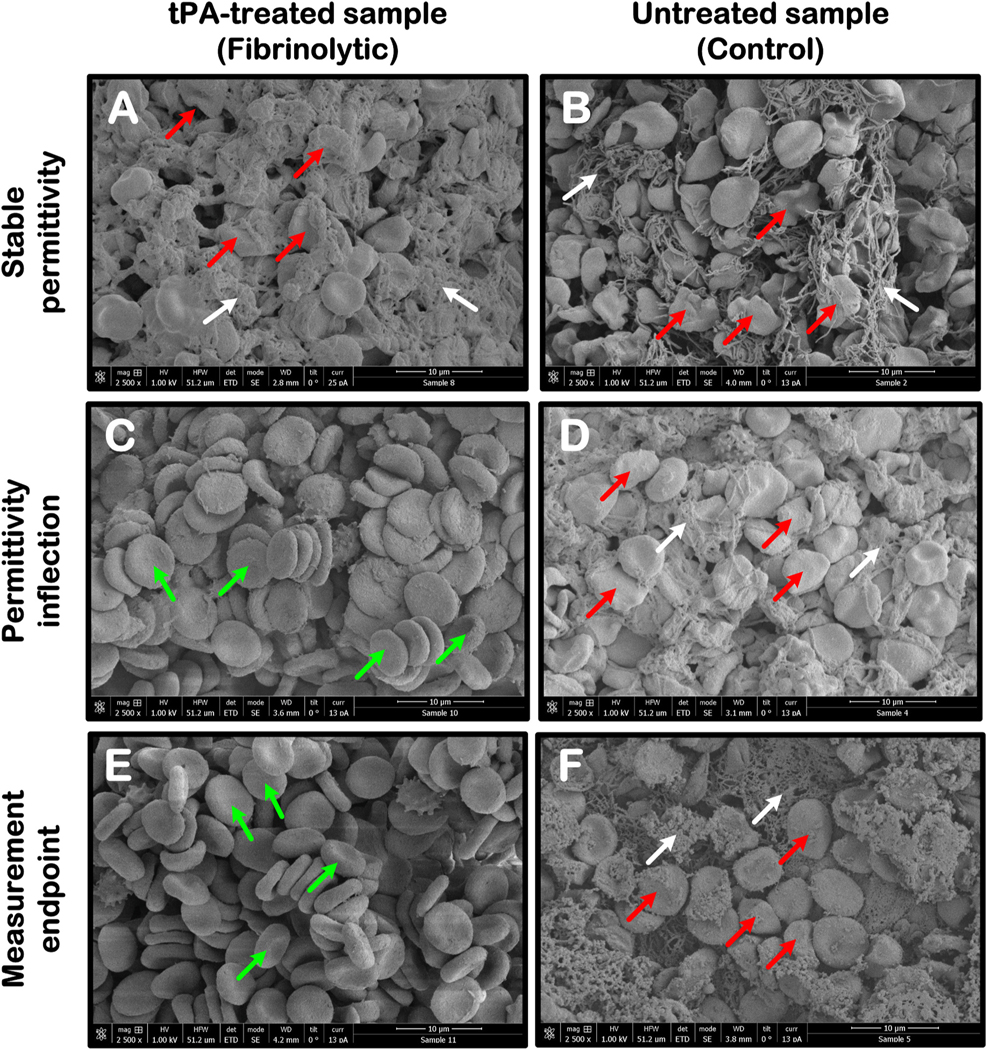
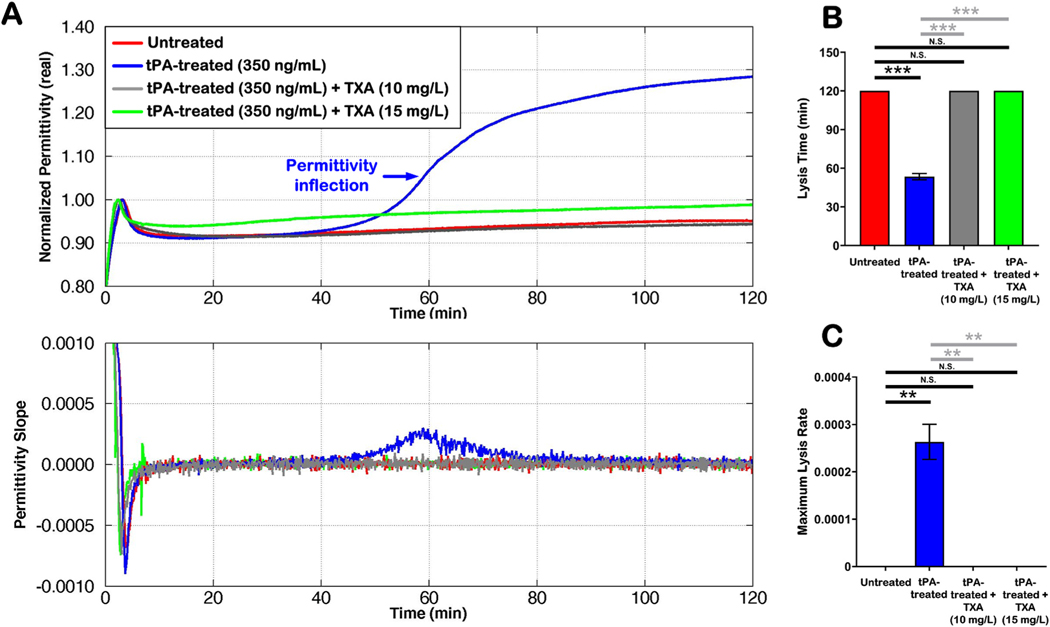
Rapid assessment of the fibrinolytic status in whole blood at the point-of-care/point-of-injury (POC/POI) is clinically important to guide timely management of uncontrolled bleeding in patients suffering from hyperfibrinolysis after a traumatic injury. In this work, we present a three-dimensional, parallel-plate, capacitive sensor - termed ClotChip - that measures the temporal variation in the real part of blood dielectric permittivity at 1 MHz as the sample undergoes coagulation within a microfluidic channel with <10 μL of total volume. The ClotChip sensor features two distinct readout parameters, namely, lysis time (LT) and maximum lysis rate (MLR) that are shown to be sensitive to the fibrinolytic status in whole blood. Specifically, LT identifies the time that it takes from the onset of coagulation for the fibrin clot to mostly dissolve in the blood sample during fibrinolysis, whereas MLR captures the rate of fibrin clot lysis. Our findings are validated through correlative measurements with a rotational thromboelastometry (ROTEM) assay of clot viscoelasticity, qualitative/quantitative assessments of clot stability, and scanning electron microscope imaging of clot ultrastructural changes, all in a tissue plasminogen activator (tPA)-induced fibrinolytic environment. Moreover, we demonstrate the ClotChip sensor ability to detect the hemostatic rescue that occurs when the tPA-induced upregulated fibrinolysis is inhibited by addition of tranexamic acid (TXA) - a potent antifibrinolytic drug. This work demonstrates the potential of ClotChip as a diagnostic platform for rapid POC/POI assessment of fibrinolysis-related hemostatic abnormalities in whole blood to guide therapy.
Keywords: Dielectric coagulometry; Dielectric spectroscopy; Fibrinolysis monitoring; Microfluidics; Point-of-care diagnostics; Whole blood coagulation.
Copyright © 2022 Elsevier B.V. All rights reserved.
Figures
Similar articles
-
A surface-functionalized whole blood-based dielectric microsensor for assessment of clot firmness in a fibrinolytic environment.Biosens Bioelectron. 2025 Jan 1;267:116789. doi: 10.1016/j.bios.2024.116789. Epub 2024 Sep 17. Biosens Bioelectron. 2025. PMID: 39332249
-
Assessment of whole blood coagulation with a microfluidic dielectric sensor.J Thromb Haemost. 2018 Oct;16(10):2050-2056. doi: 10.1111/jth.14244. Epub 2018 Sep 25. J Thromb Haemost. 2018. PMID: 30007048 Free PMC article.
-
ClotChip: A Microfluidic Dielectric Sensor for Point-of-Care Assessment of Hemostasis.IEEE Trans Biomed Circuits Syst. 2017 Dec;11(6):1459-1469. doi: 10.1109/TBCAS.2017.2739724. Epub 2017 Sep 12. IEEE Trans Biomed Circuits Syst. 2017. PMID: 28920906 Free PMC article.
-
Role of Plasminogen Activation System in Platelet Pathophysiology: Emerging Concepts for Translational Applications.Int J Mol Sci. 2022 May 28;23(11):6065. doi: 10.3390/ijms23116065. Int J Mol Sci. 2022. PMID: 35682744 Free PMC article. Review.
-
Hemostasis associated with abnormalities of fibrinolysis.Blood Rev. 1989 Mar;3(1):11-7. doi: 10.1016/0268-960x(89)90021-0. Blood Rev. 1989. PMID: 2650772 Review.
Cited by
-
D-DI/PLT can be a prognostic indicator for sepsis.PeerJ. 2023 Sep 5;11:e15910. doi: 10.7717/peerj.15910. eCollection 2023. PeerJ. 2023. PMID: 37692119 Free PMC article.
-
Contemporary approaches to treat people with hemophilia: what's new and what's not?Res Pract Thromb Haemost. 2025 Jan 31;9(1):102696. doi: 10.1016/j.rpth.2025.102696. eCollection 2025 Jan. Res Pract Thromb Haemost. 2025. PMID: 40084158 Free PMC article. Review.
References
-
- Asami K, Sekine K, 2007. Dielectric modeling of erythrocyte aggregation in blood. J. Phys. D Appl. Phys 40, 2197–2204. 10.1088/0022-3727/40/7/051. - DOI
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
