

Age-dependent and sex-dependent disparity in mortality in patients with adrenal incidentalomas and autonomous cortisol secretion: an international, retrospective, cohort study
- PMID: 35533704
- PMCID: PMC9679334
- DOI: 10.1016/S2213-8587(22)00100-0
Age-dependent and sex-dependent disparity in mortality in patients with adrenal incidentalomas and autonomous cortisol secretion: an international, retrospective, cohort study
Abstract
Background: The association between cortisol secretion and mortality in patients with adrenal incidentalomas is controversial. We aimed to assess all-cause mortality, prevalence of comorbidities, and occurrence of cardiovascular events in uniformly stratified patients with adrenal incidentalomas and cortisol autonomy (defined as non-suppressible serum cortisol on dexamethasone suppression testing).
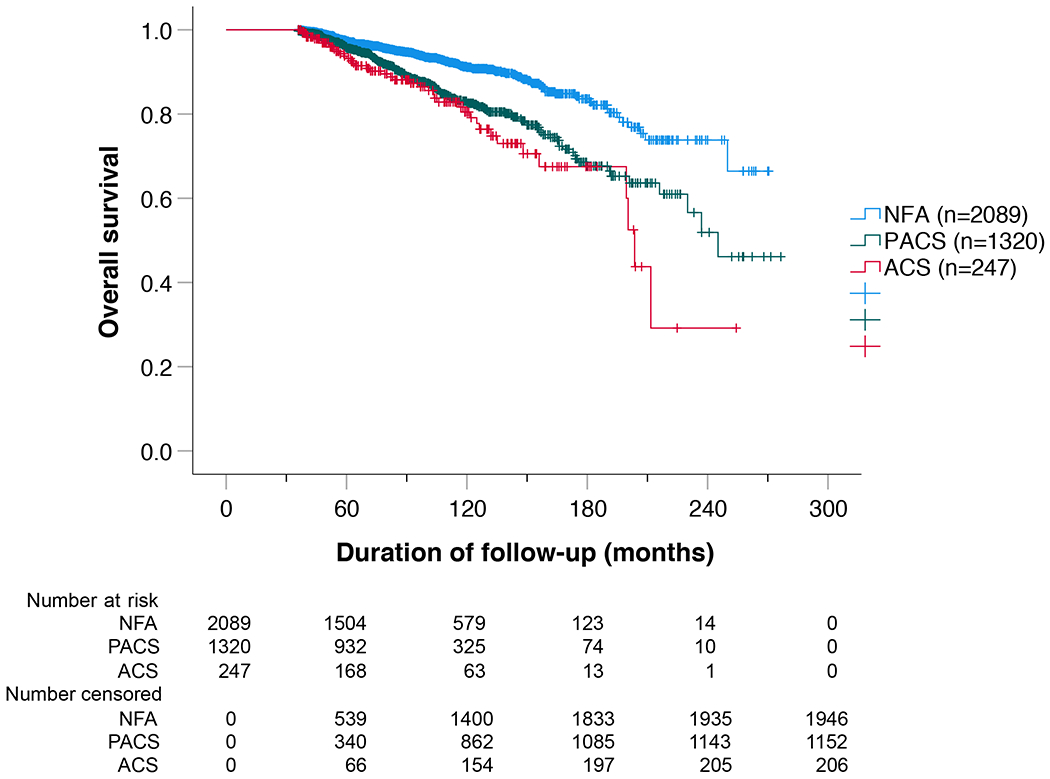
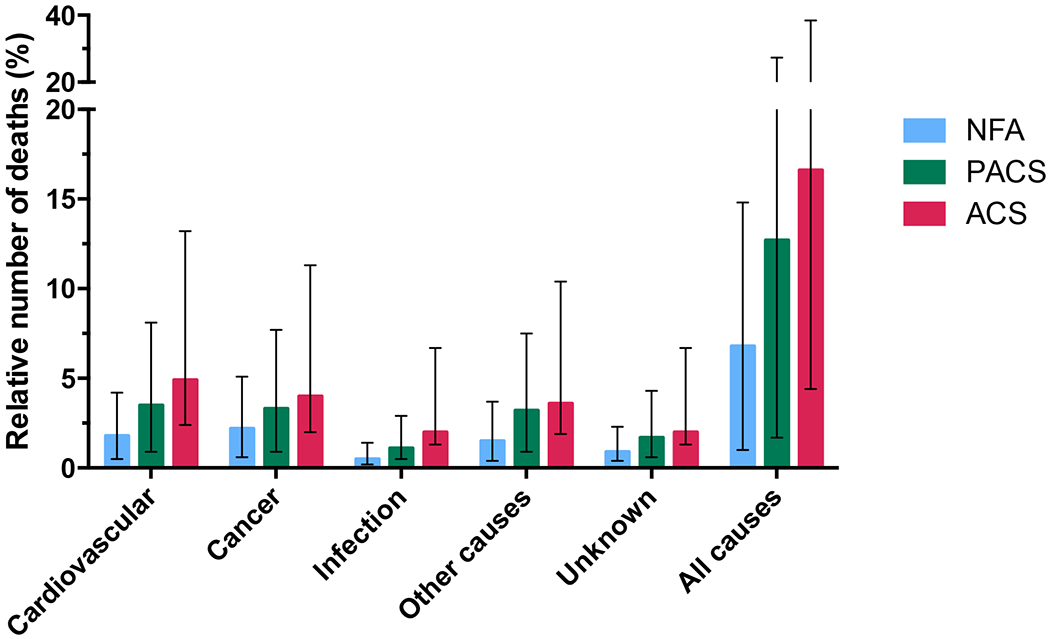
Methods: We conducted an international, retrospective, cohort study (NAPACA Outcome) at 30 centres in 16 countries. Eligible patients were aged 18 years or older with an adrenal incidentaloma (diameter ≥1 cm) detected between Jan 1, 1996, and Dec 31, 2015, and availability of a 1 mg dexamethasone suppression test result from the time of the initial diagnosis. Patients with clinically apparent hormone excess, active malignancy, or follow-up of less than 36 months were excluded. Patients were stratified according to the 0800-0900 h serum cortisol values after an overnight 1 mg dexamethasone suppression test; less than 50 nmol/L was classed as non-functioning adenoma, 50-138 nmol/L as possible autonomous cortisol secretion, and greater than 138 nmol/L as autonomous cortisol secretion. The primary endpoint was all-cause mortality. Secondary endpoints were the prevalence of cardiometabolic comorbidities, cardiovascular events, and cause-specific mortality. The primary and secondary endpoints were assessed in all study participants.
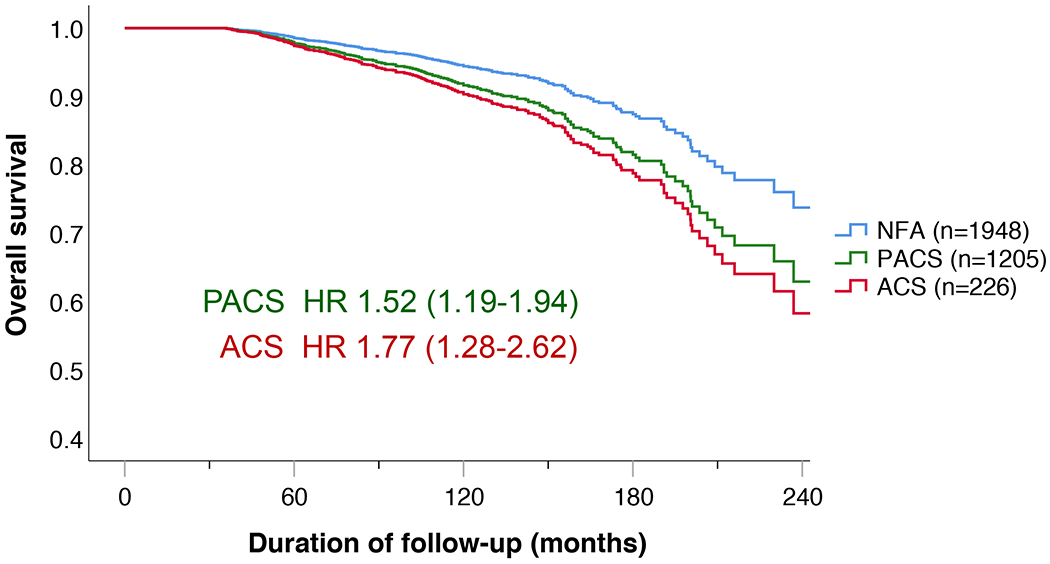
Findings: Of 4374 potentially eligible patients, 3656 (2089 [57·1%] with non-functioning adenoma, 1320 [36·1%] with possible autonomous cortisol secretion, and 247 [6·8%] with autonomous cortisol secretion) were included in the study cohort for mortality analysis (2350 [64·3%] women and 1306 [35·7%] men; median age 61 years [IQR 53-68]; median follow-up 7·0 years [IQR 4·7-10·2]). During follow-up, 352 (9·6%) patients died. All-cause mortality (adjusted for age, sex, comorbidities, and previous cardiovascular events) was significantly increased in patients with possible autonomous cortisol secretion (HR 1·52, 95% CI 1·19-1·94) and autonomous cortisol secretion (1·77, 1·20-2·62) compared with patients with non-functioning adenoma. In women younger than 65 years, autonomous cortisol secretion was associated with higher all-cause mortality than non-functioning adenoma (HR 4·39, 95% CI 1·93-9·96), although this was not observed in men. Cardiometabolic comorbidities were significantly less frequent with non-functioning adenoma than with possible autonomous cortisol secretion and autonomous cortisol secretion (hypertension occurred in 1186 [58·6%] of 2024 patients with non-functioning adenoma, 944 [74·0%] of 1275 with possible autonomous cortisol secretion, and 179 [75·2%] of 238 with autonomous cortisol secretion; dyslipidaemia occurred in 724 [36·2%] of 1999 patients, 547 [43·8%] of 1250, and 123 [51·9%] of 237; and any diabetes occurred in 365 [18·2%] of 2002, 288 [23·0%] of 1250, and 62 [26·7%] of 232; all p values <0·001).
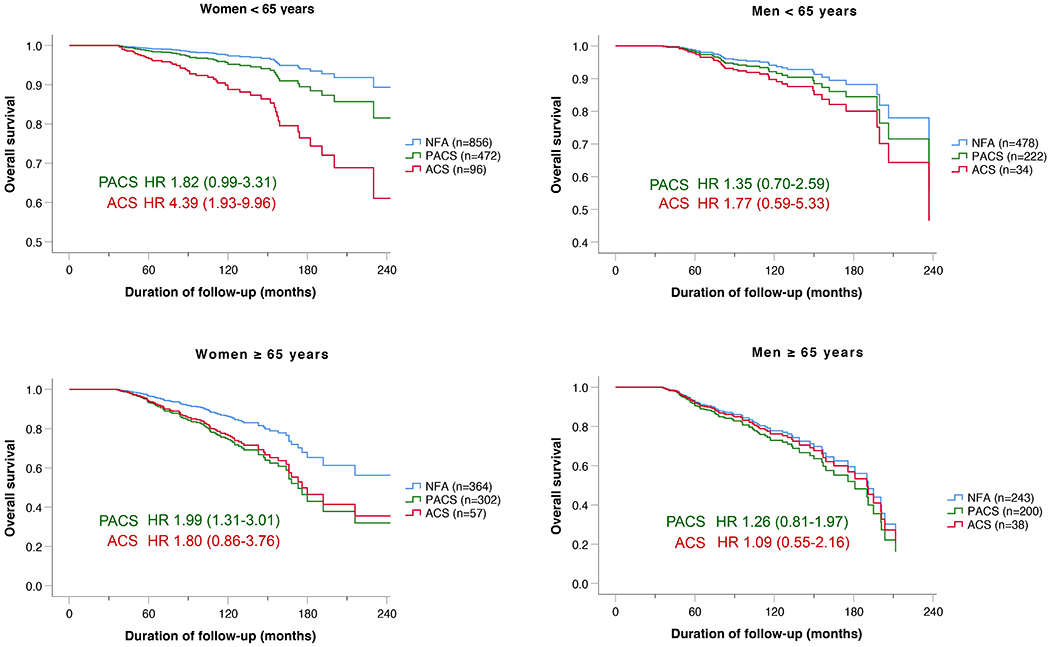
Interpretation: Cortisol autonomy is associated with increased all-cause mortality, particularly in women younger than 65 years. However, until results from randomised interventional trials are available, a conservative therapeutic approach seems to be justified in most patients with adrenal incidentaloma.
Funding: Deutsche Forschungsgemeinschaft, Associazione Italiana per la Ricerca sul Cancro, Università di Torino.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests IB has served as a consultant for Corcept Therapeutics, Sparrow Pharmaceutics, and Spruce Biosciences; was as a member of advisory or data safety monitoring boards for Adrenas Therapeutics, Recordati, and Strongbridge Biopharma (in all cases, institution fees were provided); and reports personal honoraria from Elsevier ClinicalKey. IC reports consulting fees and honoraria from HRA Pharma Rare Diseases and Recordati; was a member of advisory or data safety monitoring boards for HRA Pharma Rare Diseases and Recordati; and has participated in clinical studies from Corcept Therapeutics. ACh reports personal support for attending meetings or travel from Sanofi; personal honoraria from Ipsen; and was a member of advisory or data safety monitoring boards for Ipsen. TDe reports personal consulting fees for being a member of advisory or data safety monitoring boards for HRA Pharma Rare Diseases and Recordati; personal honoraria from Novartis; and has participated in clinical studies from Corcept Therapeutics and HRA Pharma Rare Diseases (for these, institution fees were provided). MF has participated in clinical studies from Corcept Therapeutics and HRA Pharma Rare Diseases (for these, institution fees were provided). LM was a member of the expert panel “Focus Area Adrenal and Cardiovascular Endocrinology” from the European Society of Endocrinology, and led the working group 5 of the project “CA20122—Harmonizing clinical care and research on adrenal tumours in European countries” from the European Cooperation in Science in Technology. JN-P reports grants from Diurnal Group; and has served as a consultant for and received honoraria from HRA Pharma Rare Diseases, Crinetics Pharmaceuticals, and Recordati (in all cases, institution fees were provided). CS reports consulting fees and honoraria from HRA Pharma Rare Diseases and Recordati; was a member of advisory or data safety monitoring boards for HRA Pharma Rare Diseases and Recordati; and has served as coordinator of the Pituitary Club of the Italian Society of Endocrinology. MT reports personal consulting fees (for being a member of advisory or data safety monitoring boards for Corcept Therapeutics and HRA Pharma Rare Diseases); and has participated in clinical studies from HRA Pharma Rare Diseases (for which institution fees were provided). ST reports personal support for attending meetings or travel from Ipsen, Pfizer, and Recordati; personal honoraria from Recordati; and has participated in clinical studies from Crinetics Pharmaceuticals, Novartis, and Strongbridge Biopharma. All other authors declare no competing interests.
Figures
Comment in
-
Is autonomous cortisol secretion sexually dimorphic?Lancet Diabetes Endocrinol. 2022 Jul;10(7):473-475. doi: 10.1016/S2213-8587(22)00110-3. Epub 2022 May 6. Lancet Diabetes Endocrinol. 2022. PMID: 35533705 No abstract available.
References
-
- Reimondo G, Castellano E, Grosso M, Priotto R, Puglisi S, Pia A, et al. Adrenal Incidentalomas are Tied to Increased Risk of Diabetes: Findings from a Prospective Study. The Journal of clinical endocrinology and metabolism. 2020; 105(4). - PubMed
-
- Mantero F, Terzolo M, Arnaldi G, Osella G, Masini AM, Ali A, et al. A survey on adrenal incidentaloma in Italy. Study Group on Adrenal Tumors of the Italian Society of Endocrinology. The Journal of clinical endocrinology and metabolism. 2000; 85(2): 637–44. - PubMed
-
- Cawood TJ, Hunt PJ, O’Shea D, Cole D, Soule S. Recommended evaluation of adrenal incidentalomas is costly, has high false-positive rates and confers a risk of fatal cancer that is similar to the risk of the adrenal lesion becoming malignant; time for a rethink? European journal of endocrinology / European Federation of Endocrine Societies. 2009; 161(4): 513–27. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
