

Reducing exacerbations in children and adults with primary ciliary dyskinesia using erdosteine and/or azithromycin therapy (REPEAT trial): study protocol for a multicentre, double-blind, double-dummy, 2×2 partial factorial, randomised controlled trial
- PMID: 35534039
- PMCID: PMC9086630
- DOI: 10.1136/bmjresp-2022-001236
Reducing exacerbations in children and adults with primary ciliary dyskinesia using erdosteine and/or azithromycin therapy (REPEAT trial): study protocol for a multicentre, double-blind, double-dummy, 2×2 partial factorial, randomised controlled trial
Abstract
Introduction: Primary ciliary dyskinesia (PCD) is a rare, progressive, inherited ciliopathic disorder, which is incurable and frequently complicated by the development of bronchiectasis. There are few randomised controlled trials (RCTs) involving children and adults with PCD and thus evidence of efficacy for interventions are usually extrapolated from people with cystic fibrosis. Our planned RCT seeks to address some of these unmet needs by employing a currently prescribed (but unapproved for long-term use in PCD) macrolide antibiotic (azithromycin) and a novel mucolytic agent (erdosteine). The primary aim of our RCT is to determine whether regular oral azithromycin and erdosteine over a 12-month period reduces acute respiratory exacerbations among children and adults with PCD. Our primary hypothesis is that: people with PCD who regularly use oral azithromycin and/or erdosteine will have fewer exacerbations than those receiving the corresponding placebo medications. Our secondary aims are to determine the effect of the trial medications on PCD-specific quality-of-life (QoL) and other clinical outcomes (lung function, time-to-next exacerbation, hospitalisations) and nasopharyngeal bacterial carriage and antimicrobial resistance.
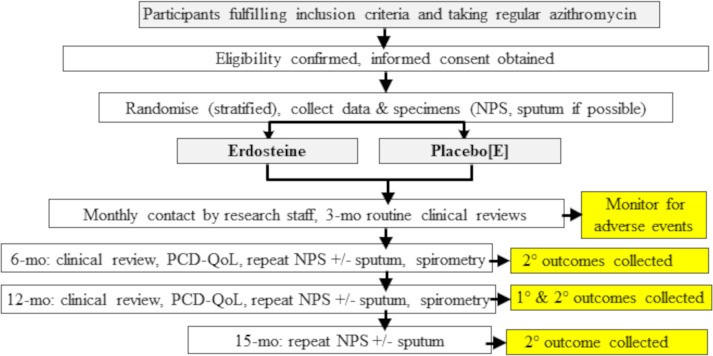
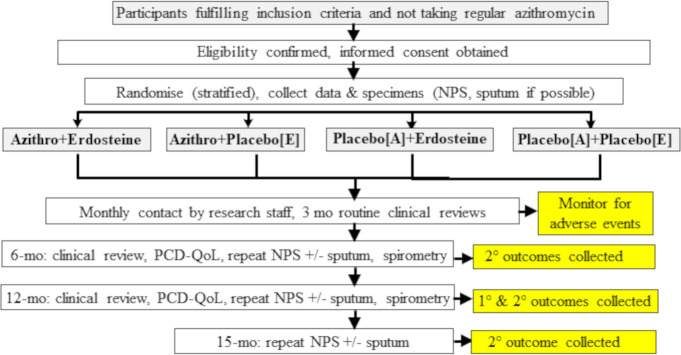
Methods and analysis: We are currently undertaking a multicentre, double-blind, double-dummy RCT to evaluate whether 12 months of azithromycin and/or erdosteine is beneficial for children and adults with PCD. We plan to recruit 104 children and adults with PCD to a parallel, 2×2 partial factorial superiority RCT at five sites across Australia. Our primary endpoint is the rate of exacerbations over 12 months. Our main secondary outcomes are QoL, lung function and nasopharyngeal carriage by respiratory bacterial pathogens and their associated azithromycin resistance.
Ethics and dissemination: Our RCT is conducted in accordance with Good Clinical Practice and the Australian legislation and National Health and Medical Research Council guidelines for ethical conduct of Research, including that for First Nations Australians.
Trial registration number: ACTRN12619000564156.
Keywords: bronchiectasis.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Erdosteine in children and adults with bronchiectasis (BETTER trial): study protocol for a multicentre, double-blind, randomised controlled trial.BMJ Open Respir Res. 2024 May 7;11(1):e002216. doi: 10.1136/bmjresp-2023-002216. BMJ Open Respir Res. 2024. PMID: 38719503 Free PMC article.
-
Azithromycin to prevent acute lower respiratory infections among Australian and New Zealand First Nations and Timorese children (PETAL trial): study protocol for a multicentre, international, double-blind, randomised controlled trial.BMJ Open. 2025 Feb 5;15(2):e097455. doi: 10.1136/bmjopen-2024-097455. BMJ Open. 2025. PMID: 39909513 Free PMC article.
-
Efficacy and safety of azithromycin maintenance therapy in primary ciliary dyskinesia (BESTCILIA): a multicentre, double-blind, randomised, placebo-controlled phase 3 trial.Lancet Respir Med. 2020 May;8(5):493-505. doi: 10.1016/S2213-2600(20)30058-8. Lancet Respir Med. 2020. PMID: 32380069 Clinical Trial.
-
Azithromycin is the answer in paediatric respiratory medicine, but what was the question?Paediatr Respir Rev. 2020 Apr;34:67-74. doi: 10.1016/j.prrv.2019.07.002. Epub 2019 Aug 16. Paediatr Respir Rev. 2020. PMID: 31629643 Review.
-
Bacteriology and treatment of infections in the upper and lower airways in patients with primary ciliary dyskinesia: adressing the paranasal sinuses.Dan Med J. 2017 May;64(5):B5361. Dan Med J. 2017. PMID: 28552099 Review.
Cited by
-
Beyond the present: current and future perspectives on the role of infections in pediatric PCD.Front Pediatr. 2025 Mar 18;13:1564156. doi: 10.3389/fped.2025.1564156. eCollection 2025. Front Pediatr. 2025. PMID: 40171169 Free PMC article. Review.
-
Erdosteine in children and adults with bronchiectasis (BETTER trial): study protocol for a multicentre, double-blind, randomised controlled trial.BMJ Open Respir Res. 2024 May 7;11(1):e002216. doi: 10.1136/bmjresp-2023-002216. BMJ Open Respir Res. 2024. PMID: 38719503 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources