

Pharmacological targeting of the tumor-immune symbiosis in glioblastoma
- PMID: 35534356
- PMCID: PMC9288491
- DOI: 10.1016/j.tips.2022.04.002
Pharmacological targeting of the tumor-immune symbiosis in glioblastoma
Abstract
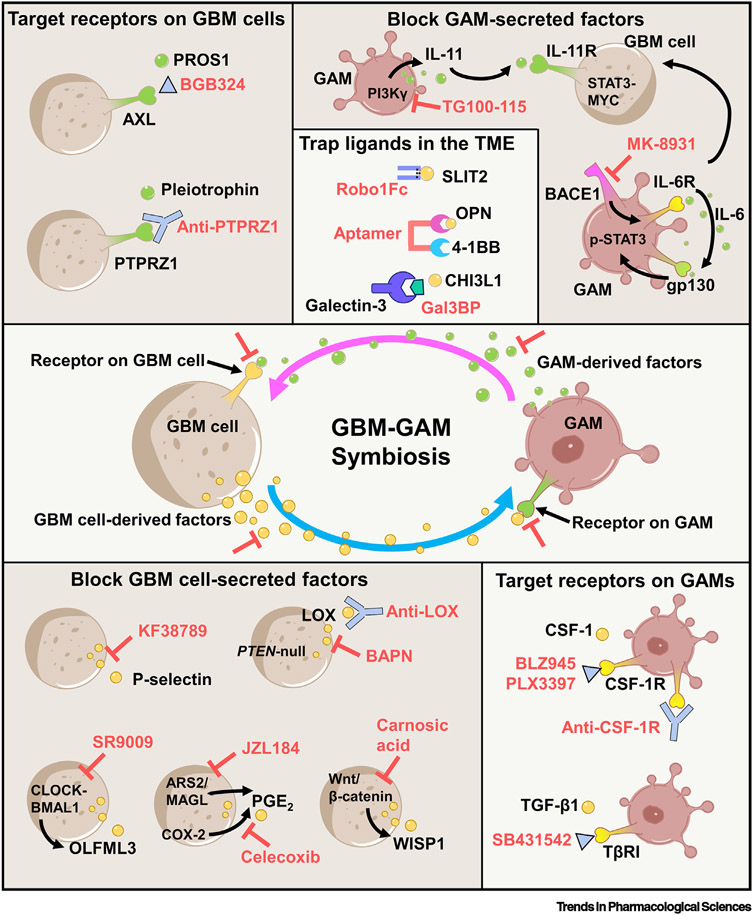
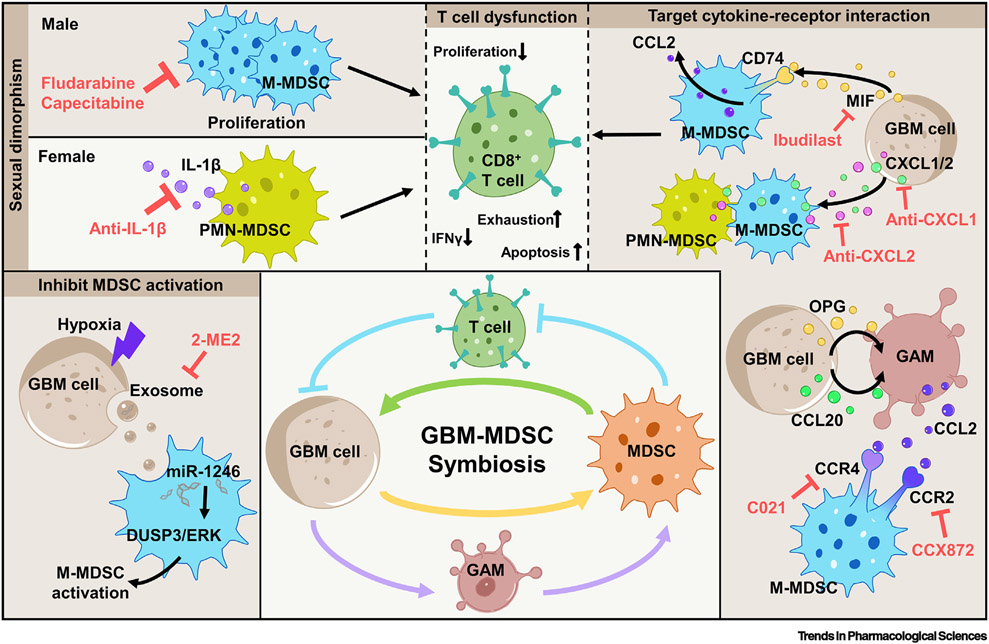
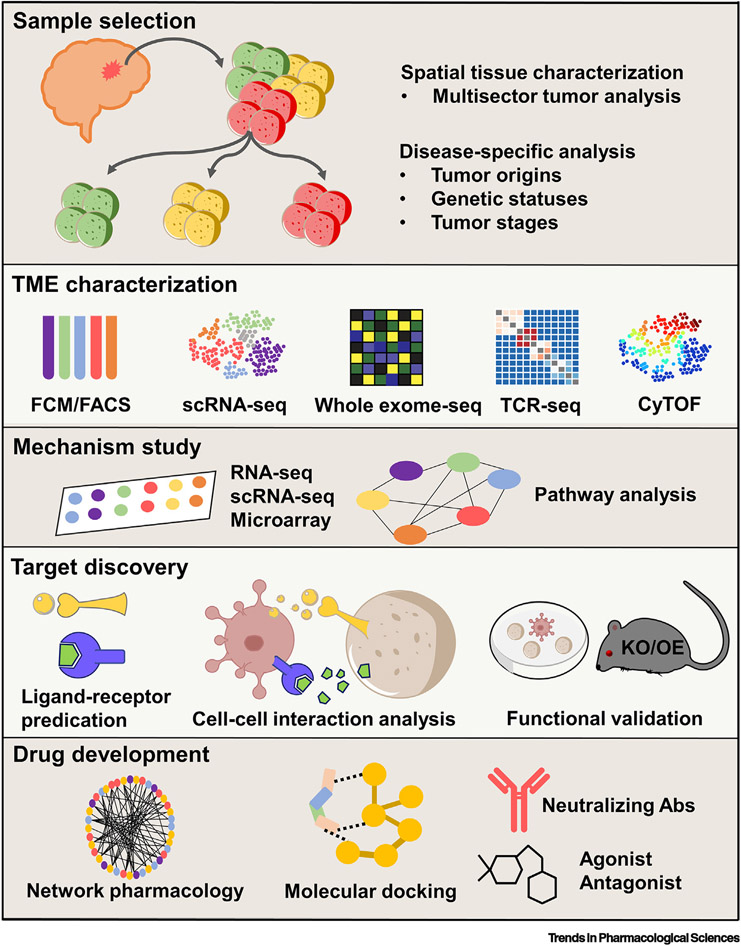
Glioblastoma (GBM) is the most common and highly lethal form of primary brain tumor in adults. The median survival of GBM patients is approximately 14-16 months despite multimodal therapies. Emerging evidence has substantiated the critical role of symbiotic interactions between GBM cells and noncancerous immune cells (e.g., myeloid cells and T cells) in regulating tumor progression and therapy resistance. Approaches to target the tumor-immune symbiosis have emerged as a promising therapeutic strategy for GBM. Here, we review the recent developments for pharmacological targeting of the GBM-immune symbiosis and highlight the role of such strategies to improve the effectiveness of immunotherapies in GBM.
Keywords: glioblastoma; immunotherapy; macrophages; microglia, MDSCs; symbiosis.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests No potential conflicts of interest were disclosed by the authors.
Figures
References
-
- Jackson CM et al. (2019) Mechanisms of immunotherapy resistance: lessons from glioblastoma. Nat. Immunol 20, 1100–1109 - PubMed
-
- Lim M et al. (2018) Current state of immunotherapy for glioblastoma. Nat. Rev. Clin. Oncol 15, 422–442 - PubMed
-
- Bejarano L et al. (2021) Therapeutic targeting of the tumor microenvironment. Cancer Discov. 11, 933–959 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
