

Reconstruction of maxillofacial bone defects using patient-specific long-lasting titanium implants
- PMID: 35534499
- PMCID: PMC9085892
- DOI: 10.1038/s41598-022-11200-0
Reconstruction of maxillofacial bone defects using patient-specific long-lasting titanium implants
Abstract
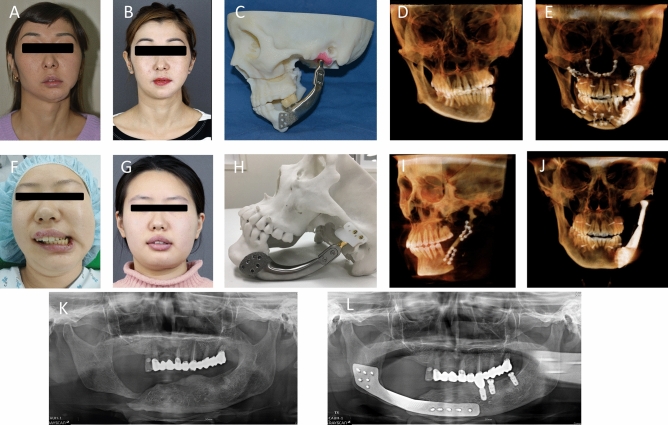
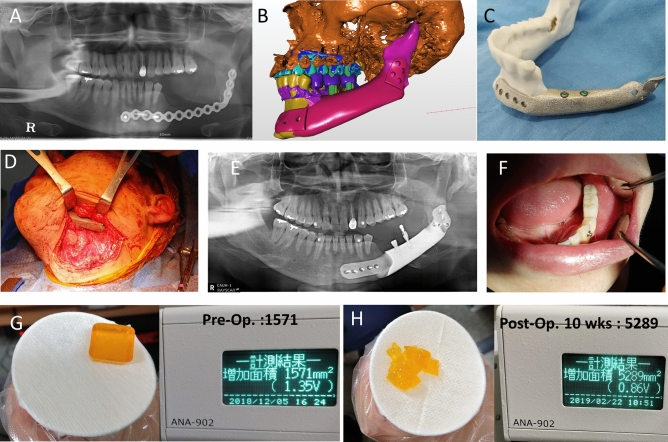
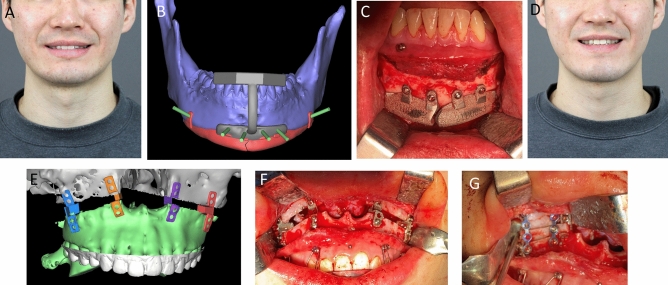
The objective of this retrospective study is to verify the effectiveness and safety of patient-specific titanium implants on maxillofacial bones, with a long-term follow-up. Total 16 patients with various maxillofacial defects underwent reconstruction using patient-specific titanium implants. Titanium implants, manufactured by electron beam melting, selective laser sintering, or milling, were inserted into the maxilla, mandible, or zygoma. Long-term follow-up (36.7 ± 20.1 months) was conducted after the surgery. Bone fusion of the titanium implant body, postoperative infection, implant malunion, functional results, patient satisfaction, subsidence, osteolysis around the implants, and complications were recorded and analyzed at the last follow-up. Of the 28 implants, only one failed to unite with the bone; therefore, revision surgery was performed. No osteolysis or subsidence around the titanium implants nor adverse events were observed; the mean VAS score for satisfaction was 9. All patients enrolled in this trial were esthetically and functionally satisfied with their surgical results, and fixation failure and esthetic dissatisfaction complications were well resolved. Patient-specific titanium showed satisfactory outcomes when used to treat various oral and maxillofacial defects. A 3D printed titanium implant can be effectively used in the reconstruction of the zygoma and mandible instead of autogenous bone without donor site morbidity.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
A Clinical Trial to Evaluate the Efficacy and Safety of 3D Printed Bioceramic Implants for the Reconstruction of Zygomatic Bone Defects.Materials (Basel). 2020 Oct 12;13(20):4515. doi: 10.3390/ma13204515. Materials (Basel). 2020. PMID: 33053855 Free PMC article.
-
Cranioplasty Enhanced by Three-Dimensional Printing: Custom-Made Three-Dimensional-Printed Titanium Implants for Skull Defects.J Craniofac Surg. 2016 Jun;27(4):943-9. doi: 10.1097/SCS.0000000000002656. J Craniofac Surg. 2016. PMID: 27192643
-
Reconstruction of mandible using a computer-designed 3D-printed patient-specific titanium implant: a case report.Oral Maxillofac Surg. 2021 Mar;25(1):103-111. doi: 10.1007/s10006-020-00889-w. Epub 2020 Jul 28. Oral Maxillofac Surg. 2021. PMID: 32725572
-
Treatment of midfacial defects using prostheses supported by ITI dental implants.Plast Reconstr Surg. 2004 Nov;114(6):1395-404. doi: 10.1097/01.prs.0000138595.86570.3e. Plast Reconstr Surg. 2004. PMID: 15509925 Review.
-
Patient-specific, printed titanium implants for reconstruction of mandibular continuity defects: A systematic review of the evidence.J Craniomaxillofac Surg. 2019 Jun;47(6):968-976. doi: 10.1016/j.jcms.2019.02.010. Epub 2019 Mar 4. J Craniomaxillofac Surg. 2019. PMID: 30885527 No abstract available.
Cited by
-
Prosthodontic rehabilitation of patients with a unilateral subtotal maxillectomy using a customised subperiosteal zygomatic implant: a post-COVID-19 mucormycosis.BMJ Case Rep. 2024 Jan 9;17(1):e258338. doi: 10.1136/bcr-2023-258338. BMJ Case Rep. 2024. PMID: 38199654
-
Balancing beauty and science: a review of facial implant materials in craniofacial surgery.Front Surg. 2024 Jan 24;11:1348140. doi: 10.3389/fsurg.2024.1348140. eCollection 2024. Front Surg. 2024. PMID: 38327548 Free PMC article. Review.
-
Morphometric analysis of the infratemporal fossa using three-dimensional (3D) digital models.Surg Radiol Anat. 2023 Jun;45(6):729-734. doi: 10.1007/s00276-023-03144-5. Epub 2023 Apr 10. Surg Radiol Anat. 2023. PMID: 37036494
-
Prevalence of metal implants among US adults aged 40 years and older.Sci Rep. 2025 Jan 2;15(1):584. doi: 10.1038/s41598-024-84340-0. Sci Rep. 2025. PMID: 39747559 Free PMC article.
-
A systematic review of implant materials for facial reconstructive and aesthetic surgery.Front Surg. 2025 Mar 28;12:1548597. doi: 10.3389/fsurg.2025.1548597. eCollection 2025. Front Surg. 2025. PMID: 40225117 Free PMC article.
References
-
- Ahmed W, Asim MA, Ehsan A, Abbas Q. Non-vascularized autogenous bone grafts for reconstruction of maxillofacial osseous defects. J. Coll. Phys. Surg. Pak. 2018;28:17–21. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
