

Investigating the appropriate adenosine deaminase cutoff value for the diagnosis of tuberculous pleural effusion in a country with decreasing TB burden
- PMID: 35534515
- PMCID: PMC9085779
- DOI: 10.1038/s41598-022-11460-w
Investigating the appropriate adenosine deaminase cutoff value for the diagnosis of tuberculous pleural effusion in a country with decreasing TB burden
Abstract
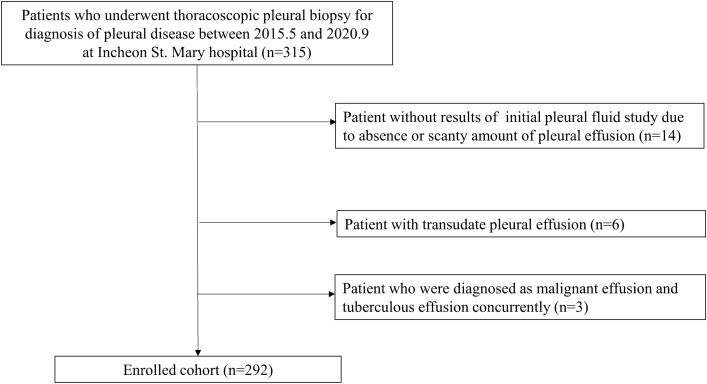
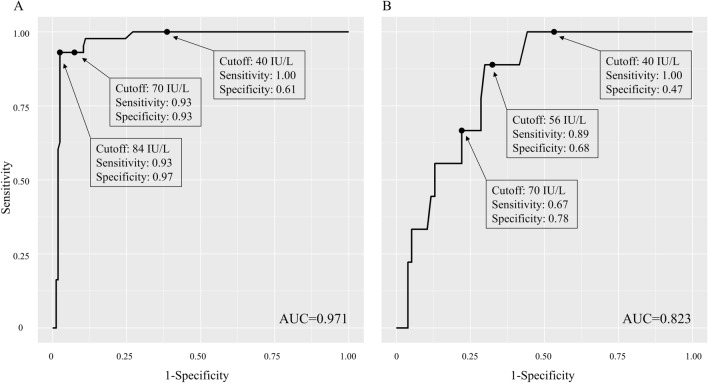
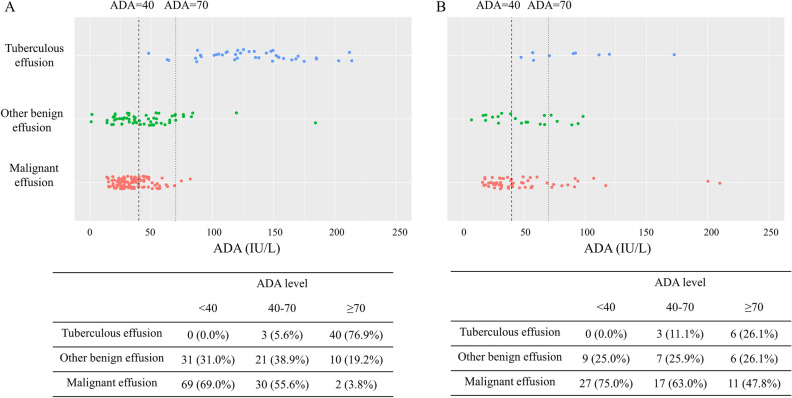
As the burden of tuberculosis (TB) in South Korea decreases while that of malignancy increases with an aging society, the composition of etiology for pleural effusion is changing. The aim of this study was to investigate the diagnostic value of adenosine deaminase (ADA) for diagnosis of tuberculous pleural effusion (TPE) in this circumstance. Medical records of patients who underwent medical thoracoscopy from May 2015 to September 2020 in Incheon St. Mary Hospital, Korea were retrospectively reviewed. TPE was diagnosed if one of the following criteria was met: (1) granuloma in pleura, (2) positive TB polymerase chain reaction or culture in pleural fluid or tissue with non-specific pathologic findings in pleura, or (3) bacteriologically confirmed pulmonary TB with non-specific pathologic findings in pleura. A total of 292 patients, including 156 with malignant pleural effusion (MPE), 52 with TPE, and 84 with other benign effusion, were analyzed. Among 206 patients with lymphocyte dominant pleural effusion, the area under receiver characteristic curve of ADA for diagnosis of TPE was 0.971. The sensitivity and specificity of a current cutoff value of 40 IU/L were 1.00 and 0.61, respectively, whereas those of a raised cutoff value of 70 IU/L were 0.93 and 0.93, respectively. Among 54 patients with ADA levels of 40-70 IU/L, 30 (55.6%) patients were diagnosed as MPE, 21 (38.9%) as other benign effusion, and only 3 (5.6%) as TPE. Caution is needed in clinical diagnosis of TPE with current ADA cutoff value in countries with decreasing TB incidence, due to many false positive cases.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- World Health Organization. Global tuberculosis report 2021 https://www.who.int/publications/i/item/9789240037021 (2021).
-
- Korea Centers for Disease Control & Prevention. Annual Report on the Notified Tuberculosis in Korea, 2020.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
