

Analyzing historical and future acute neurosurgical demand using an AI-enabled predictive dashboard
- PMID: 35534601
- PMCID: PMC9084272
- DOI: 10.1038/s41598-022-11607-9
Analyzing historical and future acute neurosurgical demand using an AI-enabled predictive dashboard
Abstract
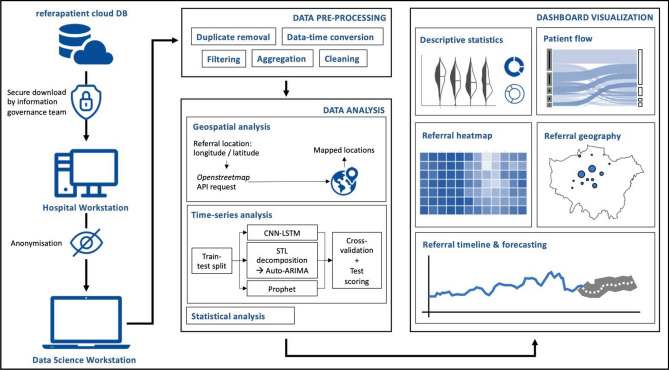
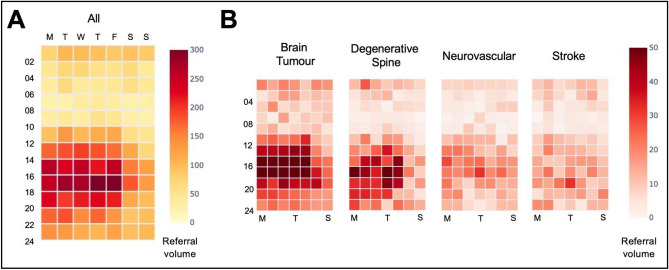
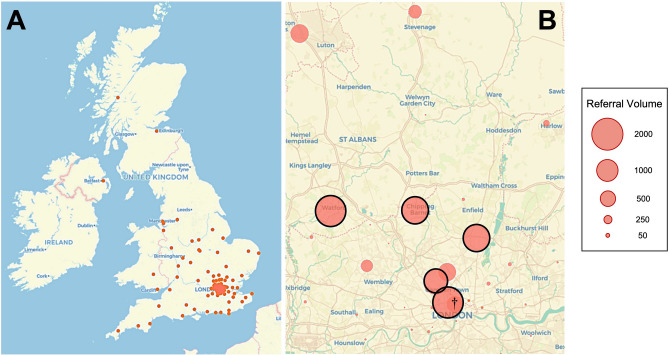
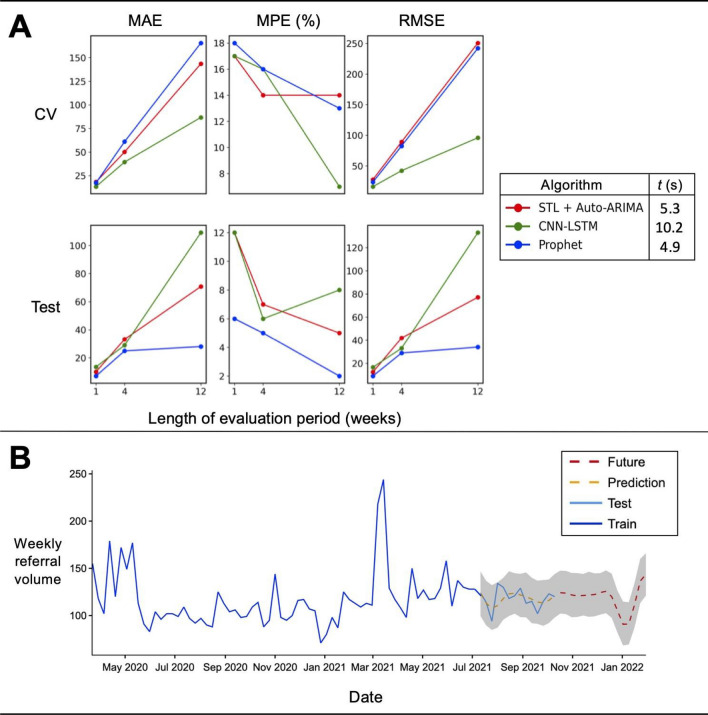
Characterizing acute service demand is critical for neurosurgery and other emergency-dominant specialties in order to dynamically distribute resources and ensure timely access to treatment. This is especially important in the post-Covid 19 pandemic period, when healthcare centers are grappling with a record backlog of pending surgical procedures and rising acute referral numbers. Healthcare dashboards are well-placed to analyze this data, making key information about service and clinical outcomes available to staff in an easy-to-understand format. However, they typically provide insights based on inference rather than prediction, limiting their operational utility. We retrospectively analyzed and prospectively forecasted acute neurosurgical referrals, based on 10,033 referrals made to a large volume tertiary neurosciences center in London, U.K., from the start of the Covid-19 pandemic lockdown period until October 2021 through the use of a novel AI-enabled predictive dashboard. As anticipated, weekly referral volumes significantly increased during this period, largely owing to an increase in spinal referrals (p < 0.05). Applying validated time-series forecasting methods, we found that referrals were projected to increase beyond this time-point, with Prophet demonstrating the best test and computational performance. Using a mixed-methods approach, we determined that a dashboard approach was usable, feasible, and acceptable among key stakeholders.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
