

Diagnostic concordance between BioFire® FilmArray® Pneumonia Panel and culture in patients with COVID-19 pneumonia admitted to intensive care units: the experience of the third wave in eight hospitals in Colombia
- PMID: 35534867
- PMCID: PMC9084542
- DOI: 10.1186/s13054-022-04006-z
Diagnostic concordance between BioFire® FilmArray® Pneumonia Panel and culture in patients with COVID-19 pneumonia admitted to intensive care units: the experience of the third wave in eight hospitals in Colombia
Abstract
Background: The detection of coinfections is important to initiate appropriate antimicrobial therapy. Molecular diagnostic testing identifies pathogens at a greater rate than conventional microbiology. We assessed both bacterial coinfections identified via culture or the BioFire® FilmArray® Pneumonia Panel (FA-PNEU) in patients infected with SARS-CoV-2 in the ICU and the concordance between these techniques.
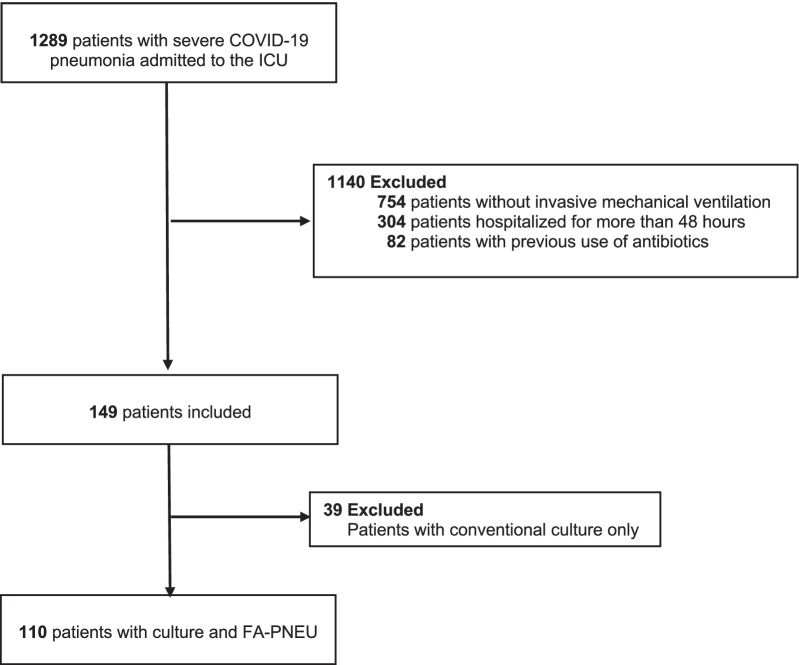
Methods: This was a prospective study of patients with SARS-CoV-2 who were hospitalized for no more than 48 h and on mechanical ventilation for no longer than 24 h in 8 ICUs in Medellín, Colombia. We studied mini-bronchoalveolar lavage or endotracheal aspirate samples processed via conventional culture and the FA-PNEU. Coinfection was defined as the identification of a respiratory pathogen using the FA-PNEU or cultures. Serum samples of leukocytes, C-reactive protein, and procalcitonin were taken on the first day of intubation. We analyzed the empirical antibiotics and the changes in antibiotic management according to the results of the FA-PNEUM and cultures.
Results: Of 110 patients whose samples underwent both methods, FA-PNEU- and culture-positive samples comprised 24.54% versus 17.27%, respectively. Eighteen samples were positive in both techniques, 82 were negative, 1 was culture-positive with a negative FA-PNEU result, and 9 were FA-PNEU-positive with negative culture. The two bacteria most frequently detected by the FA-PNEU were Staphylococcus aureus (37.5%) and Streptococcus agalactiae (20%), and those detected by culture were Staphylococcus aureus (34.78%) and Klebsiella pneumoniae (26.08%). The overall concordance was 90.1%, and when stratified by microorganism, it was between 92.7 and 100%. The positive predictive value (PPV) was between 50 and 100% and were lower for Enterobacter cloacae and Staphylococcus aureus. The negative predictive value (NPV) was high (between 99.1 and 100%); MecA/C/MREJ had a specificity of 94.55% and an NPV of 100%. The inflammatory response tests showed no significant differences between patients whose samples were positive and negative for both techniques. Sixty-one patients (55.45%) received at least one dose of empirical antibiotics.
Conclusions: The overall concordance was 90.1%, and it was between 92.7% and 100% when stratified by microorganisms. The positive predictive value was between 50 and 100%, with a very high NPV.
Keywords: Bacterial coinfection; Bacterial pneumonia; COVID-19; FilmArray; Intensive care units.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Henríquez A, Accini J, Baquero H, Molina F, Rey A, Ángel VE, et al. Clinical features and prognostic factors of adults with COVID-19 admitted to intensive care units in Colombia: a multicentre retrospective study during the first wave of the pandemic. Acta Colomb Cuid Intensivo. 2021;S0122726221000203.
-
- Langford BJ, So M, Leung V, Raybardhan S, Lo J, Kan T, et al. Predictors and microbiology of respiratory and bloodstream bacterial infection in patients with COVID-19: living rapid review update and meta-regression. Clin Microbiol Infect. 2022;28:491–501. doi: 10.1016/j.cmi.2021.11.008. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
