

Extracorporeal cardiopulmonary resuscitation in adult patients with out-of-hospital cardiac arrest: a retrospective large cohort multicenter study in Japan
- PMID: 35534870
- PMCID: PMC9088043
- DOI: 10.1186/s13054-022-03998-y
Extracorporeal cardiopulmonary resuscitation in adult patients with out-of-hospital cardiac arrest: a retrospective large cohort multicenter study in Japan
Abstract
Background: The prevalence of extracorporeal cardiopulmonary resuscitation (ECPR) in patients with out-of-hospital cardiac arrest (OHCA) has been increasing rapidly worldwide. However, guidelines or clinical studies do not provide sufficient data on ECPR practice. The aim of this study was to provide real-world data on ECPR for patients with OHCA, including details of complications.
Methods: We did a retrospective database analysis of observational multicenter cohort study in Japan. Adult patients with OHCA of presumed cardiac etiology who received ECPR between 2013 and 2018 were included. The primary outcome was favorable neurological outcome at hospital discharge, defined as a cerebral performance category of 1 or 2.
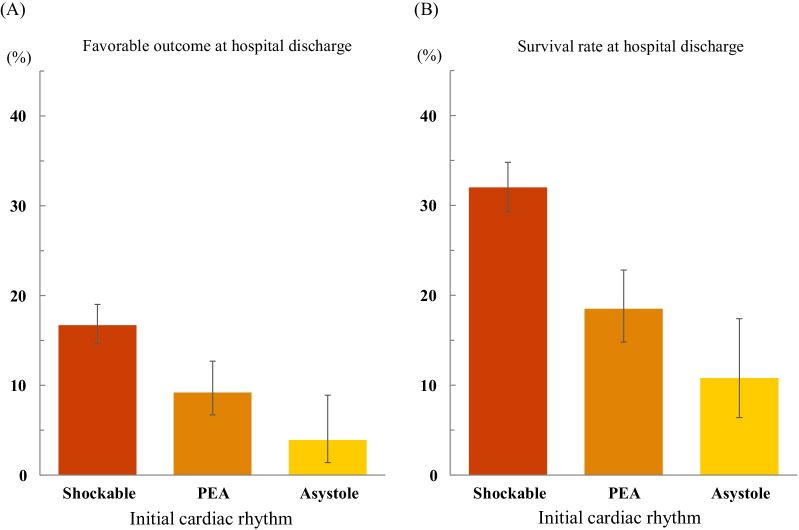
Results: A total of 1644 patients with OHCA were included in this study. The patient age was 18-93 years (median: 60 years). Shockable rhythm in the initial cardiac rhythm at the scene was 69.4%. The median estimated low flow time was 55 min (interquartile range: 45-66 min). Favorable neurological outcome at hospital discharge was observed in 14.1% of patients, and the rate of survival to hospital discharge was 27.2%. The proportions of favorable neurological outcome at hospital discharge in terms of shockable rhythm, pulseless electrical activity, and asystole were 16.7%, 9.2%, and 3.9%, respectively. Complications were observed during ECPR in 32.7% of patients, and the most common complication was bleeding, with the rates of cannulation site bleeding and other types of hemorrhage at 16.4% and 8.5%, respectively.
Conclusions: In this large cohort, data on the ECPR of 1644 patients with OHCA show that the proportion of favorable neurological outcomes at hospital discharge was 14.1%, survival rate at hospital discharge was 27.2%, and complications were observed during ECPR in 32.7%.
Keywords: Complication; Extracorporeal cardiopulmonary resuscitation; Neurological outcome; Out-of-hospital cardiac arrest; Real-world data; Survival rate.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
