

Differential prognostic burden of cardiovascular disease and lower-limb amputation on the risk of all-cause death in people with long-standing type 1 diabetes
- PMID: 35534880
- PMCID: PMC9088124
- DOI: 10.1186/s12933-022-01487-8
Differential prognostic burden of cardiovascular disease and lower-limb amputation on the risk of all-cause death in people with long-standing type 1 diabetes
Abstract
Background: Cardiovascular disease (CVD) and nontraumatic lower-limb amputation (LLA) each results in reduced life expectancy in patients with type 1 diabetes, but the differential burden between these conditions is unknown. We compared the effects of CVD and LLA on the risk of mortality in people with type 1 diabetes.
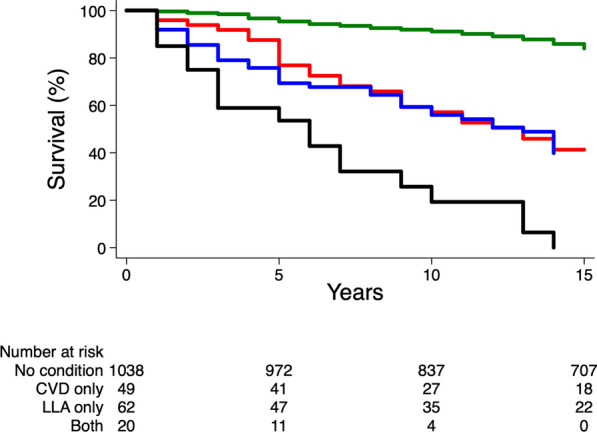
Methods: We used pooled data from the SURGENE, GENEDIAB, and GENESIS prospective cohorts. Data were divided into: 1/absence of CVD (myocardial infarction and/or stroke) nor LLA, 2/history of CVD alone without LLA, 3/LLA alone without CVD or 4/both conditions at baseline. Participants with baseline history of peripheral artery disease were excluded from groups 1 and 2. The study endpoint was any death occurring during follow-up, regardless of the causes.
Results: Among 1169 participants (male 55%, age 40 ± 13 years, diabetes duration 23 ± 11 years), CVD, LLA or both were present at baseline in 49 (4.2%), 62 (5.3%) and 20 (1.7%) subjects, respectively. All-cause death occurred in 304 (26%) participants during 17-year follow-up, corresponding to 18,426 person-years and an incidence rate of 16 (95%CI, 15-18) per 1000 person-years. The risk of death increased in individuals with baseline history of CVD (adjusted HR 2.00 [95% CI 1.34-3.01], p = 0.0008) or LLA (2.26 [1.56-3.28], p < 0.0001), versus no condition, with an additive effect in people with both conditions (5.32 [3.14-9.00], p < 0.0001). No incremental risk of death was observed in people with CVD versus LLA (0.87 [0.54-1.41]). Compared with no condition, CVD and LLA were similarly associated with reduced life expectancy during follow-up: 2.79 (95% CI 1.26-4.32) and 3.38 (1.87-4.88) years, respectively. Combined conditions expose to 7.04 (4.76-9.31) less years of life expectancy (all p < 0.0001).
Conclusions: CVD and LLA conferred a similar burden regarding mortality in type 1 diabetes population. Our findings encourage a careful consideration of people with type 1 diabetes and LLA as usually recommended for those with CVD, in terms of management of risk factors, treatments and prevention.
Keywords: Cardiovascular disease; Lower-limb amputation; Mortality; Myocardial infarction; Stroke; Type 1 diabetes mellitus.
© 2022. The Author(s).
Conflict of interest statement
L.P. reports personal fees and non-financial support from Sanofi, Novo Nordisk, Eli Lilly and MSD. VR had grants from the Servier Diabetes institute, Roche, and Merck Lipha Santé. O.B. reports personal fees and non-financial support from MSD and Sanofi. L.B. reports personal fees and non-financial support from Astra Zeneca, Bayer, BD, BMS, Boerhinger Ingelheim, MSD, Novartis, Lilly, Novo Nordisk, Roche, and Sanofi. AS has received lecturer/advisor fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Janssen, Merck Sharp and Dohme, Novartis, NovoNordisk, Sanofi and Servier. SH reports personal fees and non-financial support from Astra Zeneca, grants and personal fees from Bayer, personal fees from Boehringer Ingelheim, grants from Dinno Santé, personal fees from Eli Lilly, non-financial support from LVL, personal fees and non-financial support from MSD, personal fees from Novartis, grants from Pierre Fabre Santé, personal fees and non-financial support from Sanofi, personal fees and non-financial support from Servier, personal fees from Valbiotis. RR reports research grants from Sanofi, Novo Nordisk, and Diabnext, consulting and speakers’ bureau fees (compensation donated to the nonprofit Foundation APHP for Research) from Sanofi, Novo Nordisk, Eli Lilly, Boehringer-Ingelheim, Mundipharma, Janssen, AstraZeneca, MSD, Medtronic, and Abbott. MM is a consultant for Novo-Nordisk Algerian subsidiary, and has received personal fees from Novo-Nordisk, Merck-Sharp and Dohme, and Eli Lilly. KM reports personal fees or non-financial support from Novo Nordisk, Sanofi, Astra-Zeneca, Eli Lilly, Abbott, Boehringer-Ingelheim and LifeScan. Authors declare no other potential conflict of interest relevant to this article.
Figures
Similar articles
-
Lower-extremity amputation as a marker for renal and cardiovascular events and mortality in patients with long standing type 1 diabetes.Cardiovasc Diabetol. 2016 Jan 7;15:5. doi: 10.1186/s12933-015-0322-0. Cardiovasc Diabetol. 2016. PMID: 26743116 Free PMC article.
-
Association Between the ACE Insertion/Deletion Polymorphism and Risk of Lower-Limb Amputation in Patients With Long-Standing Type 1 Diabetes.Diabetes Care. 2022 Feb 1;45(2):407-415. doi: 10.2337/dc21-0973. Diabetes Care. 2022. PMID: 34853028
-
Exploring potential risk factors for lower limb amputation in people with diabetes-A national observational cohort study in Sweden.J Foot Ankle Res. 2024 Sep;17(3):e70005. doi: 10.1002/jfa2.70005. J Foot Ankle Res. 2024. PMID: 39217619 Free PMC article.
-
Trends in the incidence rates of lower limb amputation due to nondiabetic peripheral artery disease in a large industrial city in Western Siberia, Russia: A review from 1996 to 2019.Prosthet Orthot Int. 2022 Dec 1;46(6):619-624. doi: 10.1097/PXR.0000000000000151. Epub 2022 Jun 7. Prosthet Orthot Int. 2022. PMID: 36515907 Review.
-
Association of statin use in older people primary prevention group with risk of cardiovascular events and mortality: a systematic review and meta-analysis of observational studies.BMC Med. 2021 Jun 22;19(1):139. doi: 10.1186/s12916-021-02009-1. BMC Med. 2021. PMID: 34154589 Free PMC article.
References
-
- Rawshani A, Sattar N, Franzen S, Rawshani A, Hattersley AT, Svensson AM, et al. Excess mortality and cardiovascular disease in young adults with type 1 diabetes in relation to age at onset: a nationwide, register-based cohort study. Lancet. 2018;392(10146):477–486. doi: 10.1016/S0140-6736(18)31506-X. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
