

Effect of Sofosbuvir/Ledipasvir and Glecaprevir/Pibrentasvir on Serum Creatinine
- PMID: 35535089
- PMCID: PMC9077191
- DOI: 10.1016/j.jceh.2021.08.013
Effect of Sofosbuvir/Ledipasvir and Glecaprevir/Pibrentasvir on Serum Creatinine
Abstract
Background & objectives: There are reports of worsening renal functions with sofosbuvir, but there are no comparative data of different direct-acting antivirals (DAAs) on serum creatinine. In this retrospective cohort analysis, we examined the treatment effect of two commonly used regimens, sofosbuvir/ledipasvir (SOF/LDV) and glecaprevir/pibrentasvir (GLE/PIB), on serum creatinine.
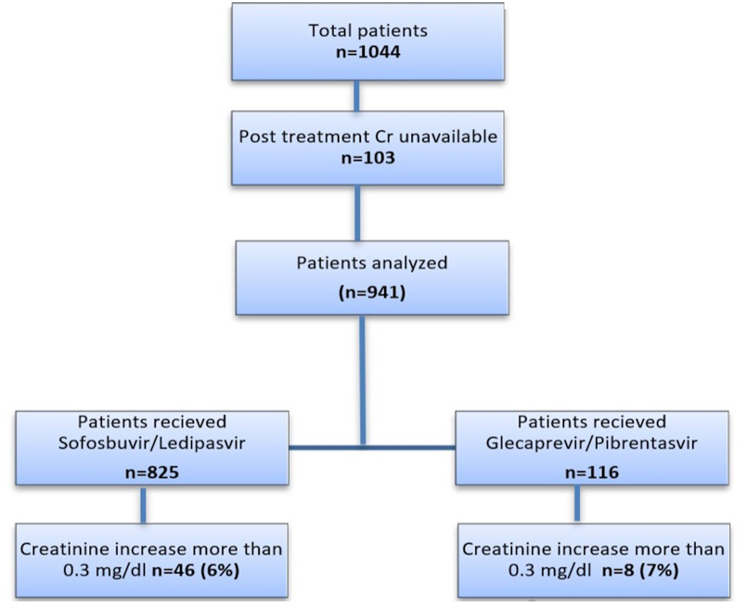
Methods: We included all patients treated with SOF/LDV (n = 825) and GLE/PIB (n = 116) between December 1, 2014, and December 31, 2018. An increase of serum creatinine ≥0.3 mg/dL was considered clinically significant. The change of creatinine values from pretreatment to posttreatment between two treatment groups was tested in unadjusted and adjusted generalized linear model, and risk factors associated with creatinine change were assessed. In addition, GLE/PIB-treated patients were matched 1:2 to SOF/LDV-treated patients using propensity scores, and then serum creatinine changes were compared.
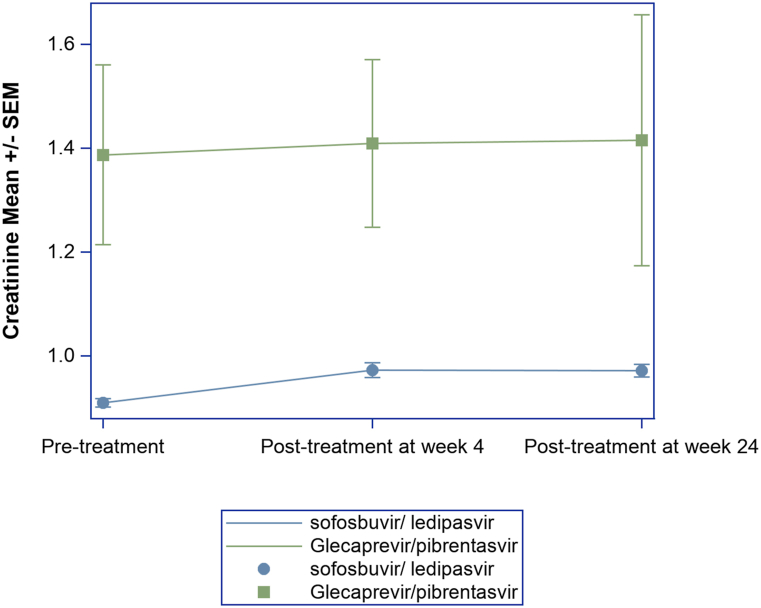
Results: The mean baseline creatinine was higher in the GLE/PIB group vs. SOF/LDV group (1.39 ± 1.86 vs. 0.91 ± 0.24, P = 0.007). When compared to baseline, serum creatinine at posttreatment week 4 was significantly higher in SOF/LDV group (0.97 ± 0.4 vs.0.91 ± 0.24, P < 0.001), but there was no significant change in the GLE/PIB group (1.41 ± 1.73 vs. 1.39 ± 1.86, P = 0.52). Overall, there was no significant change in serum creatinine between posttreatment week 4 and week 24 (P = 0.6). Clinically significant increase in serum creatinine was seen in 6% (46/825) of SOF/LDV and 7% (8/116) of GLE/PIB (P = 0.6). The unadjusted and adjusted models indicated that the changes in creatinine from baseline to posttreatment week 4 and week 24 were not associated with the type of DAA combination.
Conclusion: Treatment of chronic hepatitis C infection with both SOF/LDV and GLE/PIB regimens may result in an increase of creatinine, and 6-7% will have an increase in serum creatinine of ≥0.3 mg/dL. The increase in creatinine, however, is unrelated to the type of DAA combination.
Keywords: AKI, acute kidney injury; Cr, creatinine; DAA; DAA, direct acting antivirals; GFR, glomerular filtration rate; GLE/PIB, glecaprevir/pibrentasvir; HAART, highly active antiretroviral therapy; HCV, hepatitis C; IFN, interferon; SOF/LDV, sofosbuvir/ledipasvir; SVR, sustained virological response; TLV/BOC, telaprevir/boceprevir; direct antiviral agents; hepatitis C infection: serum creatinine.
© 2021 Indian National Association for Study of the Liver. Published by Elsevier B.V. All rights reserved.
Figures
References
LinkOut - more resources
Full Text Sources
