

Left Atrial Decompression in Pediatric Patients Supported With Extracorporeal Membrane Oxygenation for Failure to Wean From Cardiopulmonary Bypass: A Propensity-Weighted Analysis
- PMID: 35535596
- PMCID: PMC9851456
- DOI: 10.1161/JAHA.121.023963
Left Atrial Decompression in Pediatric Patients Supported With Extracorporeal Membrane Oxygenation for Failure to Wean From Cardiopulmonary Bypass: A Propensity-Weighted Analysis
Abstract
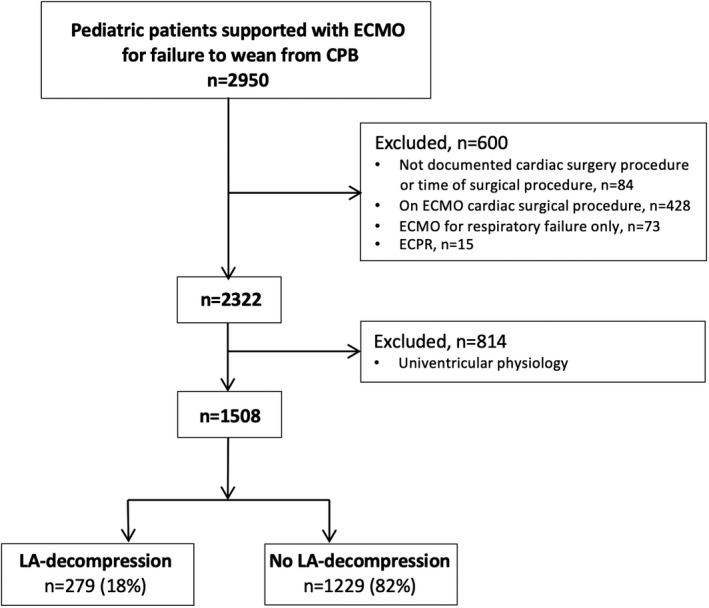
Background Left atrial (LA) decompression on extracorporeal membrane oxygenation (ECMO) can reduce left ventricular distension, allowing myocardial rest and recovery, and protect from lung injury secondary to cardiogenic pulmonary edema. However, clinical benefits remain unknown. We sought to evaluate the association between LA decompression and in-hospital adverse outcome (mortality, transplant on ECMO, or conversion to ventricular assist device) in patients who failed to wean from cardiopulmonary bypass using a propensity score to adjust for baseline differences. Methods and Results Children (aged <18 years) with biventricular physiology supported with ECMO for failure to wean from cardiopulmonary bypass after cardiac surgery from 2000 through 2016, reported to the ELSO (Extracorporeal Life Support Organization) Registry, were included. Inverse probability of treatment weighted logistic regression was used to test the association between LA decompression and in-hospital adverse outcomes. Of the 2915 patients supported with venoarterial ECMO for failure to wean from cardiopulmonary bypass, 1508 had biventricular physiology and 279 (18%) underwent LA decompression (LA+). Genetic and congenital abnormalities (P=0.001) and pulmonary hypertension (P=0.010) were less frequent and baseline arrhythmias (P=0.022) were more frequent in LA+ patients. LA+ patients had longer pre-ECMO mechanical ventilation and CBP time (P<0.001), and used aortic cross-clamp (P=0.001) more frequently. Covariates were well balanced between the propensity-weighted cohorts. In-hospital adverse outcomes occurred in 47% of LA+ patients and 51% of the others. Weighted multivariate logistic regression showed LA decompression to be protective for in-hospital adverse outcomes (adjusted odds ratio, 0.775 [95% CI, 0.644-0.932]). Conclusions LA decompression independently decreased the risk of in-hospital adverse outcome in pediatric venoarterial ECMO patients who failed to wean from cardiopulmonary bypass, suggesting that these patients may benefit from LA decompression.
Keywords: congenital heart disease; extracorporeal membrane oxygenation; failure to wean from cardiopulmonary bypass; left atrial decompression.
Figures
References
-
- Seib PM, Faulkner SC, Erickson CC, Van Devanter SH, Harrell JE, Fasules JW, Frazier EA, Morrow WR. Blade and balloon atrial septostomy for left heart decompression in patients with severe ventricular dysfunction on extracorporeal membrane oxygenation. Catheter Cardiovasc Interv. 1999;46:179–186. doi: 10.1002/(SICI)1522-726X(199902)46:2<179:AID-CCD13>3.0.CO;2-W - DOI - PubMed
-
- Johnston TA, Jaggers J, McGovern JJ, O’Laughlin MP. Bedside transseptal balloon dilation atrial septostomy for decompression of the left heart during extracorporeal membrane oxygenation. Catheter Cardiovasc Interv. 1999;46:197–199. doi: 10.1002/(SICI)1522-726X(199902)46:2<197:AID-CCD17>3.0.CO;2-G - DOI - PubMed
-
- Baruteau AE, Barnetche T, Morin L, Jalal Z, Boscamp NS, Le Bret E, Thambo JB, Vincent JA, Fraisse A, Torres AJ. Percutaneous balloon atrial septostomy on top of venoarterial extracorporeal membrane oxygenation results in safe and effective left heart decompression. Eur Heart J Acute Cardiovasc Care. 2018;7:70–79. doi: 10.1177/2048872616675485 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
