

Child Opportunity Index 2.0 and acute care utilization among children with medical complexity
- PMID: 35535923
- PMCID: PMC9254633
- DOI: 10.1002/jhm.12810
Child Opportunity Index 2.0 and acute care utilization among children with medical complexity
Abstract
Background: Disproportionately high acute care utilization among children with medical complexity (CMC) is influenced by patient-level social complexity.
Objective: The objective of this study was to determine associations between ZIP code-level opportunity and acute care utilization among CMC.
Design, setting, and participants: This cross-sectional, multicenter study used the Pediatric Health Information Systems database, identifying encounters between 2016-2019. CMC aged 28 days to <16 years with an initial emergency department (ED) encounter or inpatient/observation admission in 2016 were included in primary analyses.
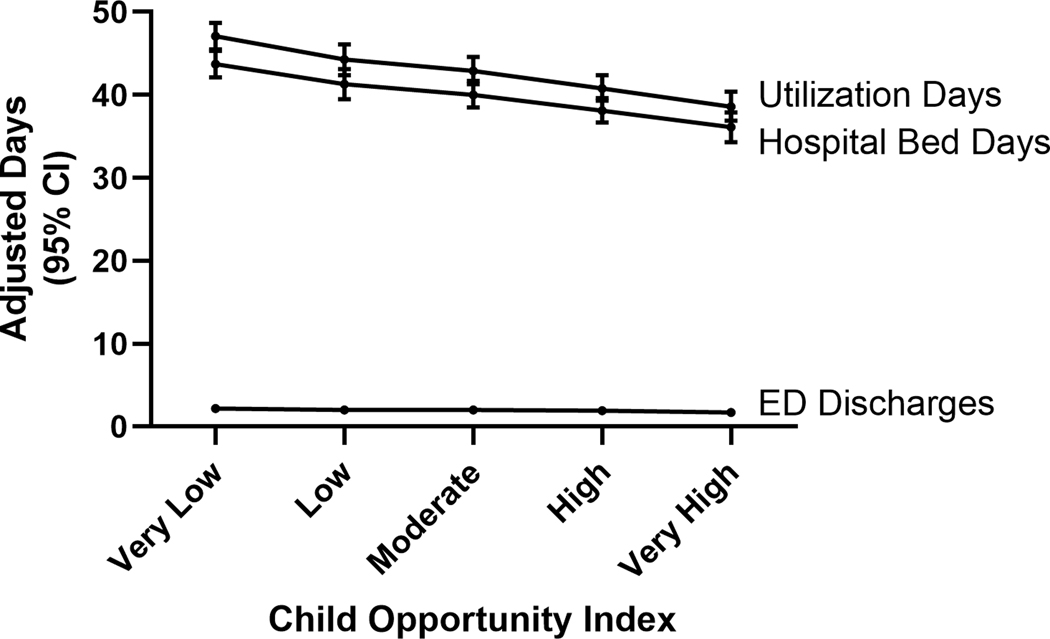
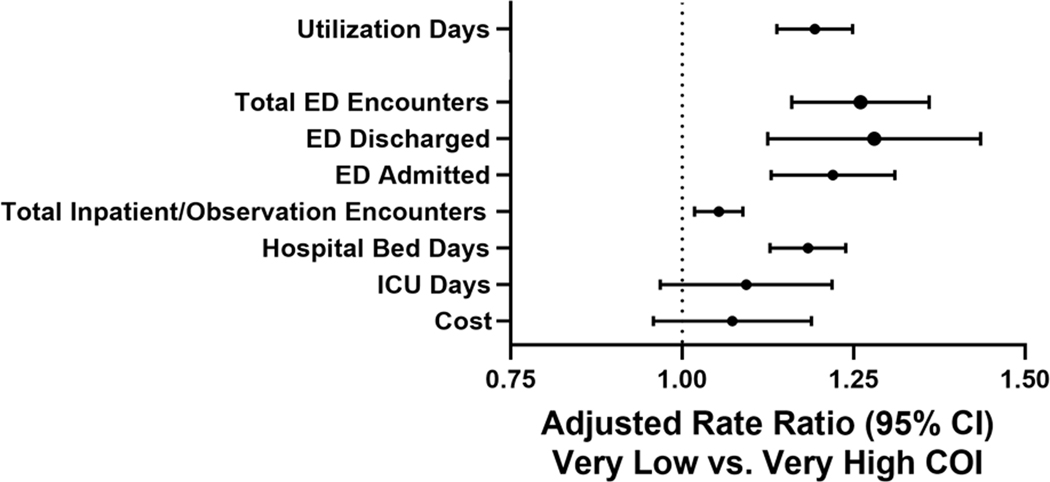
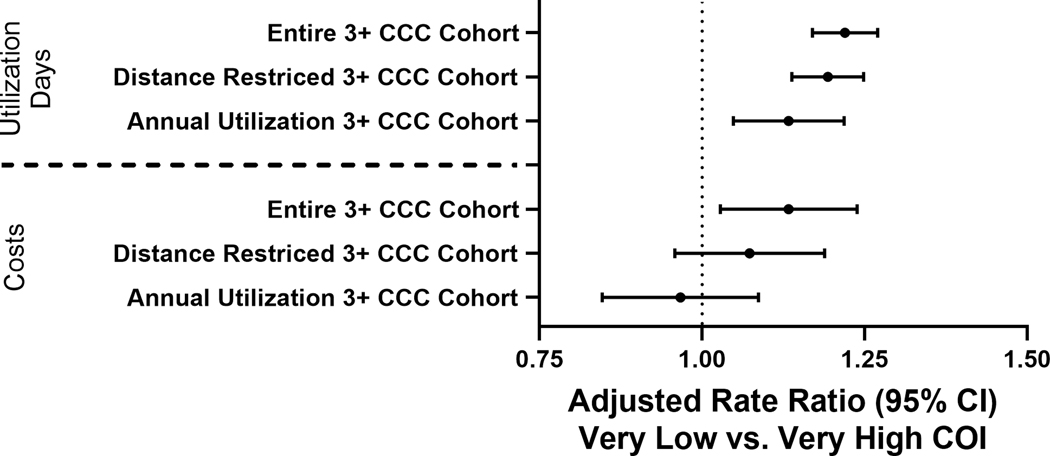
Main outcome and measures: We assessed associations between the nationally-normed, multi-dimensional, ZIP code-level Child Opportunity Index 2.0 (COI) (high COI = greater opportunity), and total utilization days (hospital bed-days + ED discharge encounters). Analyses were conducted using negative binomial generalized estimating equations, adjusting for age and distance from hospital and clustered by hospital. Secondary outcomes included intensive care unit (ICU) days and cost of care.
Results: A total of 23,197 CMC were included in primary analyses. In unadjusted analyses, utilization days decreased in a stepwise fashion from 47.1 (95% confidence interval: 45.5, 48.7) days in the lowest COI quintile to 38.6 (36.9, 40.4) days in the highest quintile (p < .001). The same trend was present across all outcome measures, though was not significant for ICU days. In adjusted analyses, patients from the lowest COI quintile utilized care at 1.22-times the rate of those from the highest COI quintile (1.17, 1.27).
Conclusions: CMC from low opportunity ZIP codes utilize more acute care. They may benefit from hospital and community-based interventions aimed at equitably improving child health outcomes.
© 2022 Society of Hospital Medicine.
Conflict of interest statement
Figures
Comment in
-
Beyond the hospital walls-Addressing social complexity in children with medical complexity.J Hosp Med. 2022 Apr;17(4):320-321. doi: 10.1002/jhm.12809. Epub 2022 Mar 21. J Hosp Med. 2022. PMID: 35535941 No abstract available.
References
-
- Fritz CQ, Thomas J, Gambino J, Torok M, Brittan MS. Prevalence of Social Risks on Inpatient Screening and Their Impact on Pediatric Care Use. Hospital pediatrics. 2020;10(10):859–866. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
