

Family Input for Quality and Safety (FIQS): Using mobile technology for in-hospital reporting from families and patients
- PMID: 35535946
- PMCID: PMC12179642
- DOI: 10.1002/jhm.2777
Family Input for Quality and Safety (FIQS): Using mobile technology for in-hospital reporting from families and patients
Abstract
Objective: Despite three decades of effort, ensuring inpatient safety remains elusive. Patients and family members are a potential source of safety observations, but systems gathering these are limited. Our goal was to test a system to gather safety observations from hospitalized patients and their family members via a real-time mobile health tool.
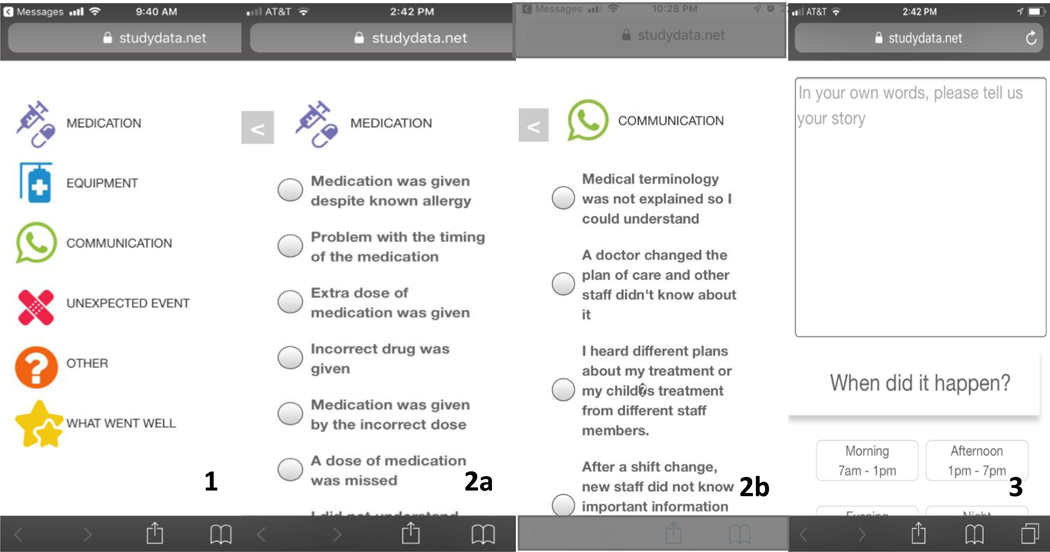
Methods: We developed a mobile-responsive website for reporting safety observations. We piloted the tool during June 2017-April 2018 on the medical-surgical unit of a children's hospital. Participants were English-speaking family members and patients ≥13 years. We sent a daily text with a website link. We assessed: (1) face validity by comparing observations to incident reporting (IR) criteria and to hospital IRs and (2) associations between the number of safety observations/100 patient-days and participant characteristics using Poisson regression.
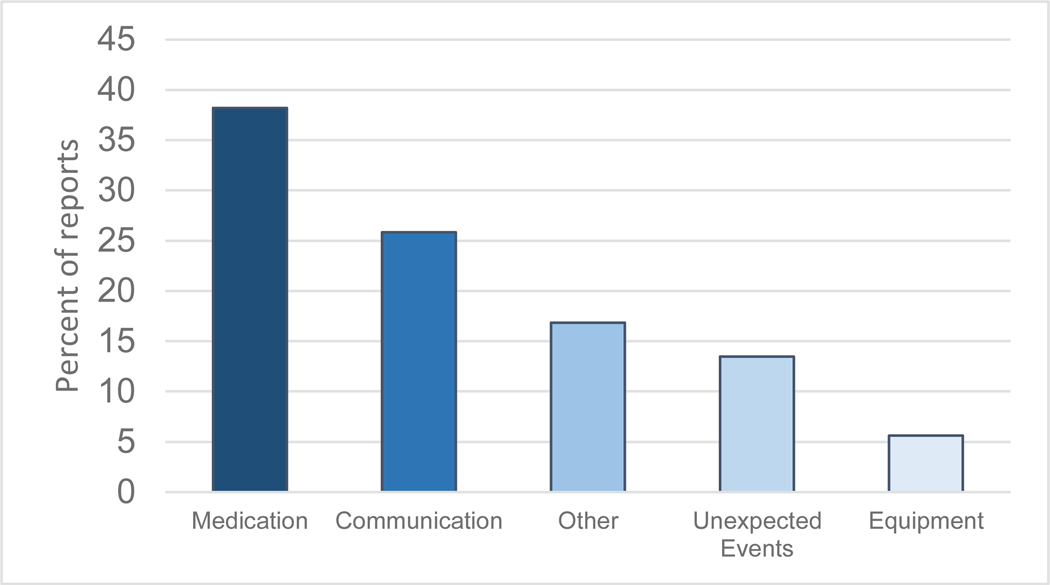
Results: We enrolled 235 patients (43.8% of 537 reviewed for eligibility), resulting in 8.15 safety reports/100 patient-days, most frequently regarding medications (29% of reports) and communication (20% of reports). Fifty-one (40% of 125) met IR criteria; only one (1.1%) had been reported via the IR system. Latinx participants submitted fewer observations than White participants (3.9 vs. 10.1, p = .002); participants with more prior hospitalizations submitted more observations (p < .001). In adjusted analyses, including measures of preference in decision making, and patient activation, the difference between Latinx and White participants diminished substantially (6.4 vs. 11.3, p = .16).
Conclusions: We demonstrated the feasibility of real-time patient and family-member technology-enabled safety observation reporting and elicited reports not otherwise identified. Variation in reporting may potentially exacerbate disparities in safety if not addressed.
© 2022 Society of Hospital Medicine.
Conflict of interest statement
Figures
References
-
- James JT. A new, evidence-based estimate of patient harms associated with hospital care. J Patient Saf. 2013;9(3):122–128. - PubMed
-
- Classen DC, Resar R, Griffin F, et al. ‘Global trigger tool’ shows that adverse events in hospitals may be ten times greater than previously measured. Health Aff (Millwood). 2011;30(4):581–589. - PubMed
-
- Shekelle PG, Pronovost PJ, Wachter RM, et al. Advancing the science of patient safety. Ann Intern Med. 2011;154(10):693–696. - PubMed
-
- Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med. 2010;363(22):2124–2134. - PubMed
-
- Stockwell DC, Bisarya H, Classen DC, et al. A trigger tool to detect harm in pediatric inpatient settings. Pediatrics. 2015;135(6):1036–1042. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
