

Cardioprotective effect of silicon-built restraint device (ASD), for left ventricular remodeling in rat heart failure model
- PMID: 35536369
- PMCID: PMC9090860
- DOI: 10.1007/s10856-022-06663-6
Cardioprotective effect of silicon-built restraint device (ASD), for left ventricular remodeling in rat heart failure model
Abstract
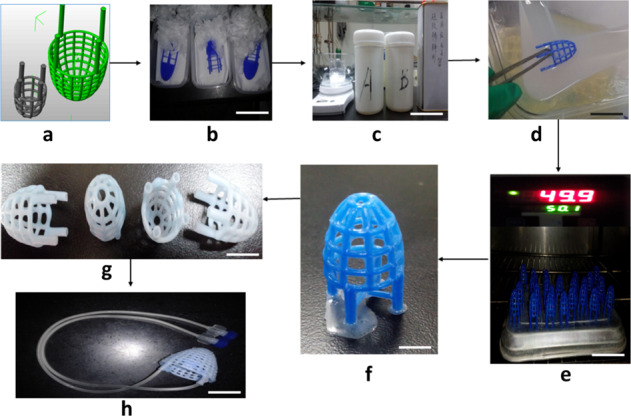
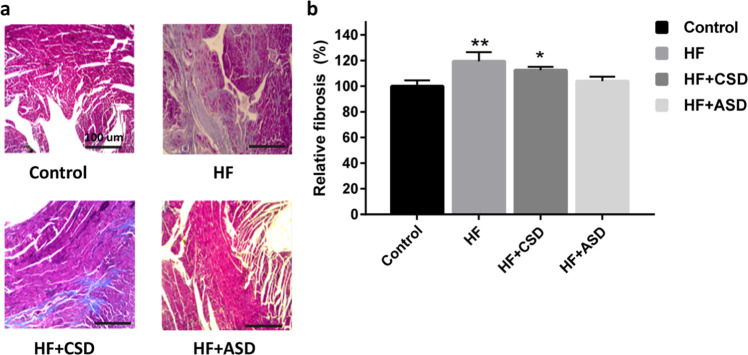
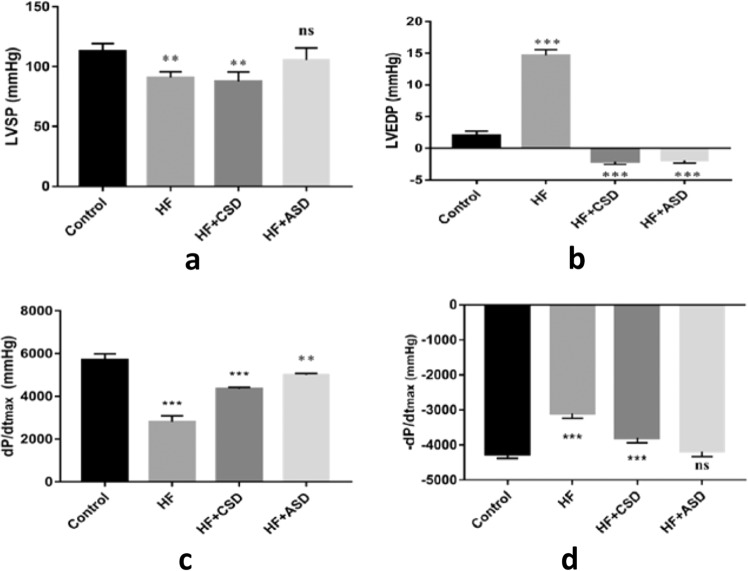
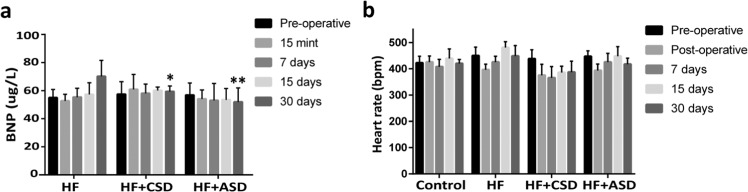
This study aims to evaluate the feasibility and cardio-protective effects of biocompatible silicon-built restraint device (ASD) in the rat's heart failure (HF) model. The performance and compliance characteristics of the ASD device were assessed in vitro by adopting a pneumatic drive and ball burst test. Sprague-Dawley (SD) rats were divided into four groups (n = 6); control, HF, HF + CSD, and HF + ASD groups, respectively. Heart failure was developed by left anterior descending (LAD) coronary artery ligation in all groups except the control group. The ASD and CSD devices were implanted in the heart of HF + ASD and HF + CSD groups, respectively. The ASD's functional and expansion ability was found to be safe and suitable for attenuating ventricular remodeling. ASD-treated rats showed normal heart rhythm, demonstrated by smooth -ST and asymmetrical T-wave. At the same time, hemodynamic parameters of the HF + ASD group improved systolic and diastolic functions, reducing ventricular wall stress, which indicated reverse remodeling. The BNP values were reduced in the HF + ASD group, which confirmed ASD feasibility and reversed remodeling at a molecular level. Furthermore, the HF + ASD group with no fibrosis suggests that ASD has significant curative effects on the heart muscles. In conclusion, ASD was found to be a promising restraint therapy than the previously standard restraint therapies. Stepwise ASD fabrication process (a) 3D computer model of ASD was generated by using Rhinoceros 5.0 software (b) 3D blue wax model of ASD (c) Silicon was prepared by mixing the solutions (as per manufacturer instruction) (d) Blue wax model of ASD was immersed into liquid Silicon (e) ASD model was put into the oven for 3 hours at 50 °C. (f) Blue wax started melting from the ASD model (g) ASD model was built from pure silicon (h) Two access lines were linked to the ASD device, which was connected with an implantable catheter (Port-a-cath), scale bar 100 µm. (Nikon Ldx 2.0).
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Cardiac support device (ASD) delivers bone marrow stem cells repetitively to epicardium has promising curative effects in advanced heart failure.Biomed Microdevices. 2018 May 12;20(2):40. doi: 10.1007/s10544-018-0282-8. Biomed Microdevices. 2018. PMID: 29754170
-
A novel ventricular restraint device (ASD) repetitively deliver Salvia miltiorrhiza to epicardium have good curative effects in heart failure management.Biomed Pharmacother. 2017 Nov;95:701-710. doi: 10.1016/j.biopha.2017.07.126. Epub 2017 Sep 5. Biomed Pharmacother. 2017. PMID: 28886530
-
Kidney-tonifying blood-activating decoction delays ventricular remodeling in rats with chronic heart failure by regulating gut microbiota and metabolites and p38 mitogen-activated protein kinase/p65 nuclear factor kappa-B/aquaporin-4 signaling pathway.J Ethnopharmacol. 2024 Aug 10;330:118110. doi: 10.1016/j.jep.2024.118110. Epub 2024 Apr 3. J Ethnopharmacol. 2024. PMID: 38580189
-
The promising future of ventricular restraint therapy for the management of end-stage heart failure.Biomed Pharmacother. 2018 Mar;99:25-32. doi: 10.1016/j.biopha.2018.01.003. Epub 2018 Jan 8. Biomed Pharmacother. 2018. PMID: 29324309 Review.
-
Cardio-supportive devices (VRD & DCC device) and patches for advanced heart failure: A review, summary of state of the art and future directions.Biomed Pharmacother. 2018 Jun;102:41-54. doi: 10.1016/j.biopha.2018.03.049. Epub 2018 Mar 15. Biomed Pharmacother. 2018. PMID: 29549728 Review.
Cited by
-
Control of the post-infarct immune microenvironment through biotherapeutic and biomaterial-based approaches.Drug Deliv Transl Res. 2023 Jul;13(7):1983-2014. doi: 10.1007/s13346-023-01290-2. Epub 2023 Feb 10. Drug Deliv Transl Res. 2023. PMID: 36763330 Free PMC article. Review.
References
-
- Heart failure—incidence and survival. N Engl J Med. 2003;348. p. 660. - PubMed
-
- Jhund PS, Macintyre K, Simpson CR, Lewsey JD, Stewart S, Redpath A, et al. Long-term trends in first hospitalization for heart failure and subsequent survival between 1986 and 2003: a population study of 5.1 million people. Circulation. 2009;119:515–23. doi: 10.1161/CIRCULATIONAHA.108.812172. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
