

Association Between Surgery Preference and Receipt in Ductal Carcinoma In Situ After Breast Magnetic Resonance Imaging: An Ancillary Study of the ECOG-ACRIN Cancer Research Group (E4112)
- PMID: 35536580
- PMCID: PMC9092204
- DOI: 10.1001/jamanetworkopen.2022.10331
Association Between Surgery Preference and Receipt in Ductal Carcinoma In Situ After Breast Magnetic Resonance Imaging: An Ancillary Study of the ECOG-ACRIN Cancer Research Group (E4112)
Abstract
Importance: Guiding treatment decisions for women with ductal carcinoma in situ (DCIS) requires understanding patient preferences and the influence of preoperative magnetic resonance imaging (MRI) and surgeon recommendation.
Objective: To identify factors associated with surgery preference and surgery receipt among a prospective cohort of women with newly diagnosed DCIS.
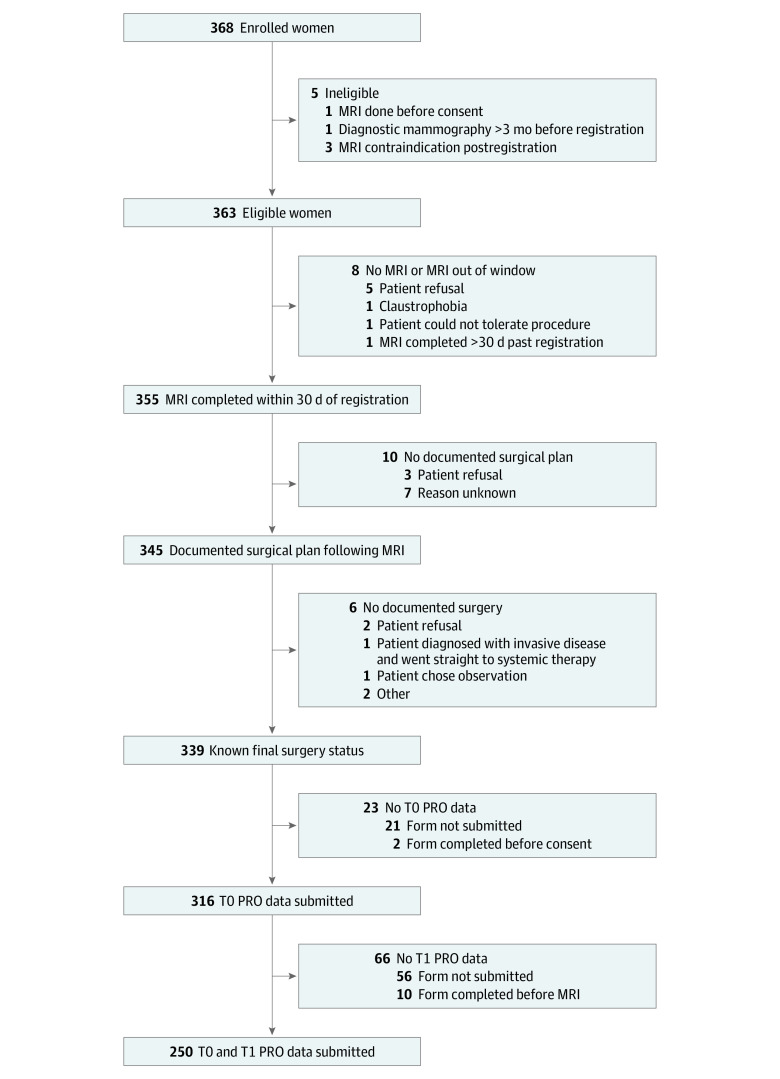
Design, setting, and participants: A prospective cohort study was conducted at 75 participating institutions, including community practices and academic centers, across the US between March 25, 2015, and April 27, 2016. Data were analyzed from August 2 to September 24, 2021. This was an ancillary study of the ECOG-ACRIN Cancer Research Group (E4112). Women with recently diagnosed unilateral DCIS who were eligible for wide local excision and had a diagnostic mammogram within 3 months of study registration were included. Participants who had documented surgery and completed the baseline patient-reported outcome questionnaires were included in this substudy.
Exposures: Women received preoperative MRI and surgeon consultation and then underwent wide local excision or mastectomy. Participants will be followed up for recurrence and overall survival for 10 years from the date of surgery.
Main outcomes and measures: Patient-reported outcome questionnaires assessed treatment goals and concerns and surgery preference before MRI and after MRI and surgeon consultation.
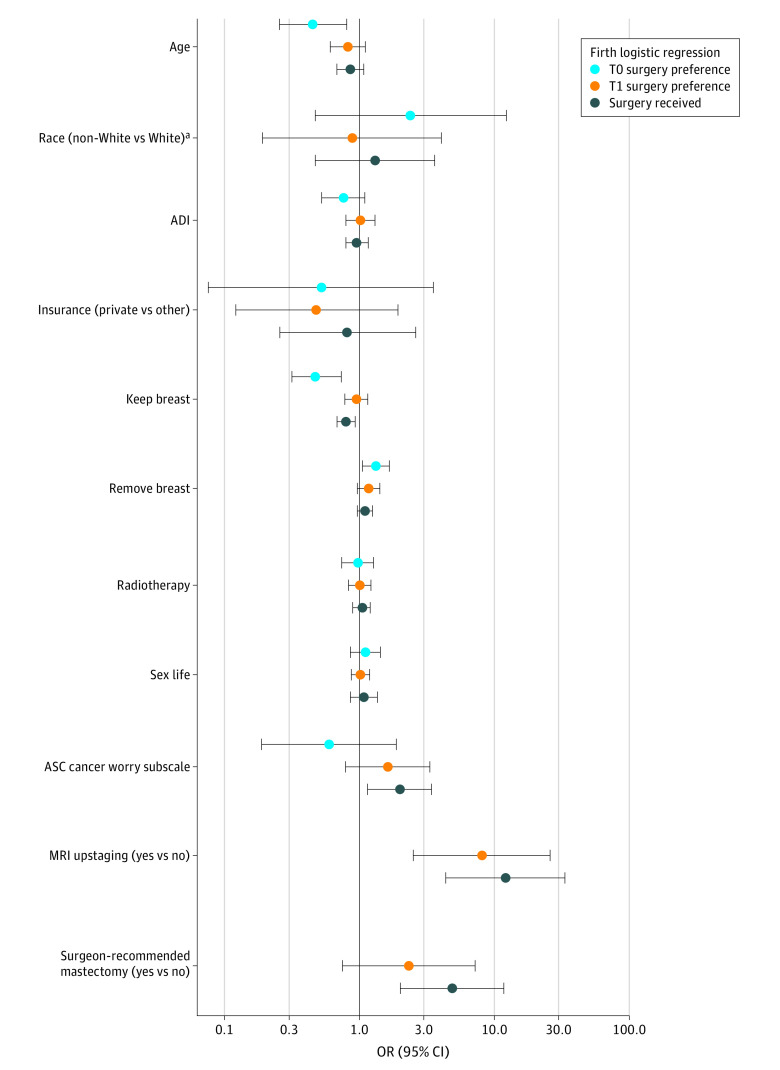
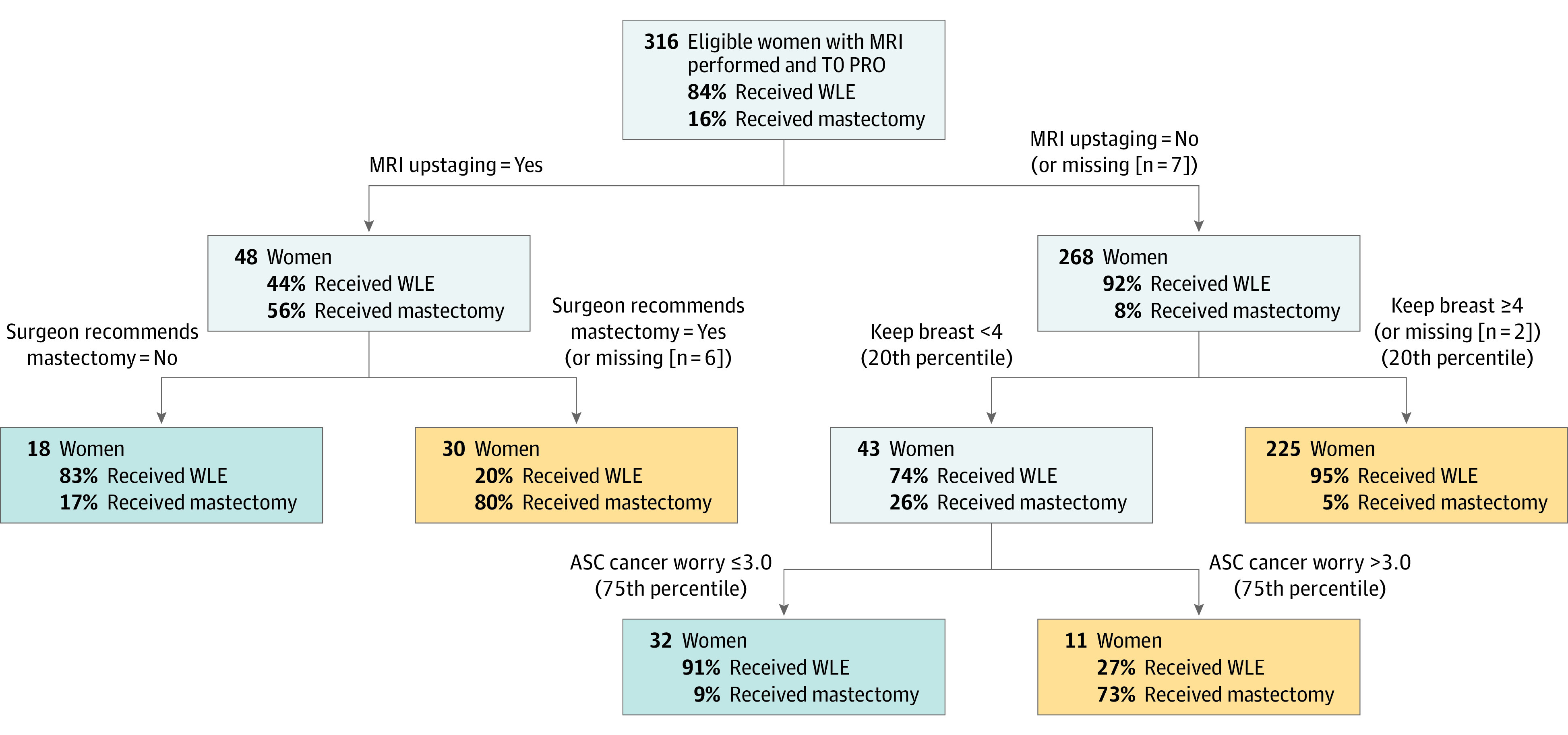
Results: Of the 368 participants enrolled 316 (86%) were included in this substudy (median [range] age, 59.5 [34-87] years; 45 women [14%] were Black; 245 [78%] were White; and 26 [8%] were of other race). Pre-MRI, age (odds ratio [OR] per 5-year increment, 0.45; 95% CI, 0.26-0.80; P = .007) and the importance of keeping one's breast (OR, 0.48; 95% CI, 0.31-0.72; P < .001) vs removal of the breast for peace of mind (OR, 1.35; 95% CI, 1.04-1.76; P = .03) were associated with surgery preference for mastectomy. After MRI and surgeon consultation, MRI upstaging (48 of 316 [15%]) was associated with patient preference for mastectomy (OR, 8.09; 95% CI, 2.51-26.06; P < .001). The 2 variables with the highest ORs for initial receipt of mastectomy were MRI upstaging (OR, 12.08; 95% CI, 4.34-33.61; P < .001) and surgeon recommendation (OR, 4.85; 95% CI, 1.99-11.83; P < .001).
Conclusions and relevance: In this cohort study, change in patient preference for DCIS surgery and surgery received were responsive to MRI results and surgeon recommendation. These data highlight the importance of ensuring adequate information and ongoing communication about the clinical significance of MRI findings and the benefits and risks of available treatment options.
Conflict of interest statement
Figures
Similar articles
-
Preoperative breast MRI positively impacts surgical outcomes of needle biopsy-diagnosed pure DCIS: a patient-matched analysis from the MIPA study.Eur Radiol. 2024 Jun;34(6):3970-3980. doi: 10.1007/s00330-023-10409-5. Epub 2023 Nov 24. Eur Radiol. 2024. PMID: 37999727 Free PMC article.
-
Patient-Reported Testing Burden of Breast Magnetic Resonance Imaging Among Women With Ductal Carcinoma In Situ: An Ancillary Study of the ECOG-ACRIN Cancer Research Group (E4112).JAMA Netw Open. 2021 Nov 1;4(11):e2129697. doi: 10.1001/jamanetworkopen.2021.29697. JAMA Netw Open. 2021. PMID: 34726748 Free PMC article.
-
Preoperative Breast MRI for Newly Diagnosed Ductal Carcinoma in Situ: Imaging Features and Performance in a Multicenter Setting (ECOG-ACRIN E4112 Trial).Radiology. 2021 Oct;301(1):66-77. doi: 10.1148/radiol.2021204743. Epub 2021 Aug 3. Radiology. 2021. PMID: 34342501 Free PMC article.
-
Association of Magnetic Resonance Imaging and a 12-Gene Expression Assay With Breast Ductal Carcinoma In Situ Treatment.JAMA Oncol. 2019 Jul 1;5(7):1036-1042. doi: 10.1001/jamaoncol.2018.6269. JAMA Oncol. 2019. PMID: 30653209 Free PMC article. Clinical Trial.
-
Meta-analysis of the effect of preoperative breast MRI on the surgical management of ductal carcinoma in situ.Br J Surg. 2015 Jul;102(8):883-93. doi: 10.1002/bjs.9797. Epub 2015 Apr 28. Br J Surg. 2015. PMID: 25919321 Review.
Cited by
-
Oncoplastic Breast Surgery versus Conservative Mastectomy in the Management of Large Ductal Carcinoma In Situ (DCIS): Surgical, Oncological, and Patient-Reported Outcomes.Cancers (Basel). 2022 Nov 16;14(22):5624. doi: 10.3390/cancers14225624. Cancers (Basel). 2022. PMID: 36428718 Free PMC article.
-
Quality of life issues in patients with ductal carcinoma in situ: a systematic review.Support Care Cancer. 2024 Oct 1;32(10):695. doi: 10.1007/s00520-024-08864-x. Support Care Cancer. 2024. PMID: 39352516
-
Quality of Life Among Patients With Ductal Carcinoma In Situ.JAMA Netw Open. 2025 Jul 1;8(7):e2518887. doi: 10.1001/jamanetworkopen.2025.18887. JAMA Netw Open. 2025. PMID: 40608342 Free PMC article. Clinical Trial.
-
Ethical dilemmas surrounding patients´ "unwise" treatment preferences and suboptimal decision quality: case series of three renal cell carcinoma patients who developed local recurrences after non-guideline-concordant care choices.Pan Afr Med J. 2024 Oct 18;49:45. doi: 10.11604/pamj.2024.49.45.42047. eCollection 2024. Pan Afr Med J. 2024. PMID: 39867546 Free PMC article.
-
Preoperative breast MRI positively impacts surgical outcomes of needle biopsy-diagnosed pure DCIS: a patient-matched analysis from the MIPA study.Eur Radiol. 2024 Jun;34(6):3970-3980. doi: 10.1007/s00330-023-10409-5. Epub 2023 Nov 24. Eur Radiol. 2024. PMID: 37999727 Free PMC article.
References
-
- American Cancer Society . Breast Cancer Facts & Figures 2019-2020. American Cancer Society Inc; 2019.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
