

Attributable Mortality of Ventilator-associated Pneumonia Among Patients with COVID-19
- PMID: 35537122
- PMCID: PMC9887408
- DOI: 10.1164/rccm.202202-0357OC
Attributable Mortality of Ventilator-associated Pneumonia Among Patients with COVID-19
Abstract
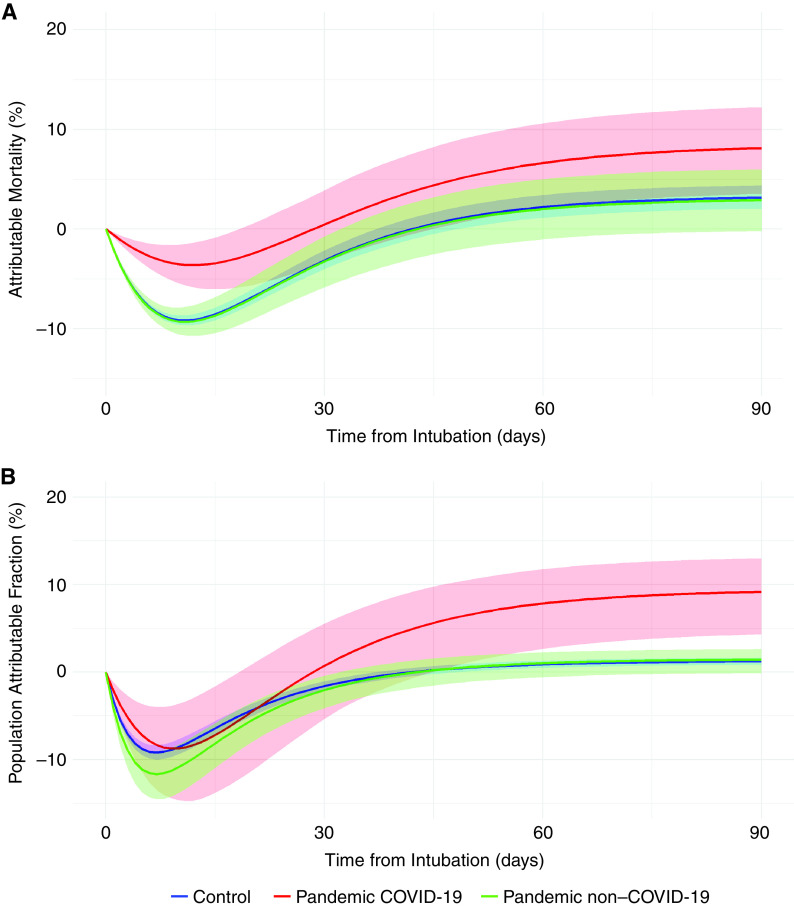
Rationale: Patients with a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection are at higher risk of ventilator-associated pneumonia (VAP) and may have an increased attributable mortality (increased or decreased risk of death if VAP occurs in a patient) and attributable fraction (proportion of deaths that are attributable to an exposure) of VAP-related mortality compared with subjects without coronavirus disease (COVID-19). Objectives: Estimation of the attributable mortality of the VAP among patients with COVID-19. Methods: Using the REA-REZO surveillance network, three groups of adult medical ICU patients were computed: control group (patients admitted between 2016 and 2019; prepandemic patients), pandemic COVID-19 group (PandeCOV+), and pandemic non-COVID-19 group (PandeCOV-) admitted during 2020. The primary outcome was the estimation of attributable mortality and attributable fraction related to VAP in these patients. Using multistate modeling with causal inference, the outcomes related to VAP were also evaluated. Measurements and Main Results: A total of 64,816 patients were included in the control group, 7,442 in the PandeCOV- group, and 1,687 in the PandeCOV+ group. The incidence of VAP was 14.2 (95% confidence interval [CI], 13.9 to 14.6), 18.3 (95% CI, 17.3 to 19.4), and 31.9 (95% CI, 29.8 to 34.2) per 1,000 ventilation-days in each group, respectively. Attributable mortality at 90 days was 3.15% (95%, CI, 2.04% to 3.43%), 2.91% (95% CI, -0.21% to 5.02%), and 8.13% (95% CI, 3.54% to 12.24%), and attributable fraction of mortality at 90 days was 1.22% (95% CI, 0.83 to 1.63), 1.42% (95% CI, -0.11% to 2.61%), and 9.17% (95% CI, 3.54% to 12.24%) for the control, PandeCOV-, and PandeCOV+ groups, respectively. Except for the higher risk of developing VAP, the PandeCOV- group shared similar VAP characteristics with the control group. PandeCOV+ patients were at lower risk of death without VAP (hazard ratio, 0.62; 95% CI, 0.52 to 0.74) than the control group. Conclusions: VAP-attributable mortality was higher for patients with COVID-19, with more than 9% of the overall mortality related to VAP.
Keywords: COVID-19; attributable mortality; population attributable fraction; ventilator-associated pneumonia.
Figures
Comment in
-
What COVID-19 Has Taught Us: Ventilator-associated Pneumonia Is Back!Am J Respir Crit Care Med. 2022 Jul 15;206(2):132-134. doi: 10.1164/rccm.202204-0799ED. Am J Respir Crit Care Med. 2022. PMID: 35579660 Free PMC article. No abstract available.
-
Causal Inference and Ventilator-associated Pneumonia-attributable Mortality in COVID-19: On Painting Bull's-Eyes and Dotting i's.Am J Respir Crit Care Med. 2023 Mar 1;207(5):630-631. doi: 10.1164/rccm.202211-2137LE. Am J Respir Crit Care Med. 2023. PMID: 36473272 Free PMC article. No abstract available.
References
-
- Coronavirus disease (COVID-19) situation reports https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio....
-
- Abrams D, Agerstrand C, Beitler JR, Karagiannidis C, Madahar P, Yip NH, et al. Risks and benefits of ultra-lung-protective invasive mechanical ventilation strategies with a focus on extracorporeal support. Am J Respir Crit Care Med . 2022;205:873–882. - PubMed
-
- Costa ELV, Slutsky AS, Brochard LJ, Brower R, Serpa-Neto A, Cavalcanti AB, et al. Ventilatory variables and mechanical power in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med . 2021;204:303–311. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
