

Visualization and Quantification of the Unrepaired Complete Atrioventricular Canal Valve Using Open-Source Software
- PMID: 35537615
- PMCID: PMC9452462
- DOI: 10.1016/j.echo.2022.04.015
Visualization and Quantification of the Unrepaired Complete Atrioventricular Canal Valve Using Open-Source Software
Abstract
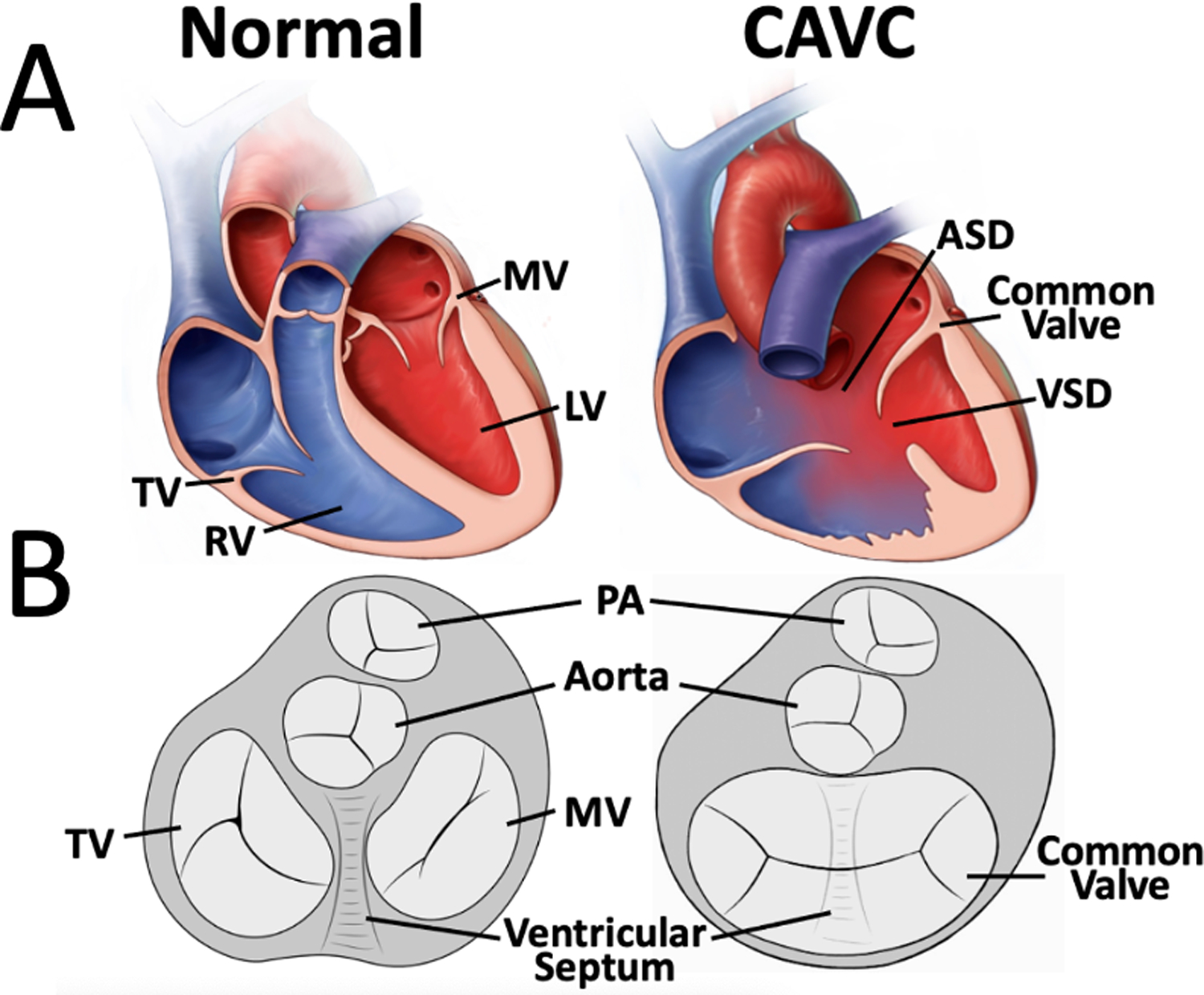
Background: Repair of complete atrioventricular canal (CAVC) is often complicated by residual left atrioventricular valve regurgitation. The structure of the mitral and tricuspid valves in biventricular hearts has previously been shown to be associated with valve dysfunction. However, the three-dimensional (3D) structure of the entire unrepaired CAVC valve has not been quantified. Understanding the 3D structure of the CAVC may inform optimized repair.
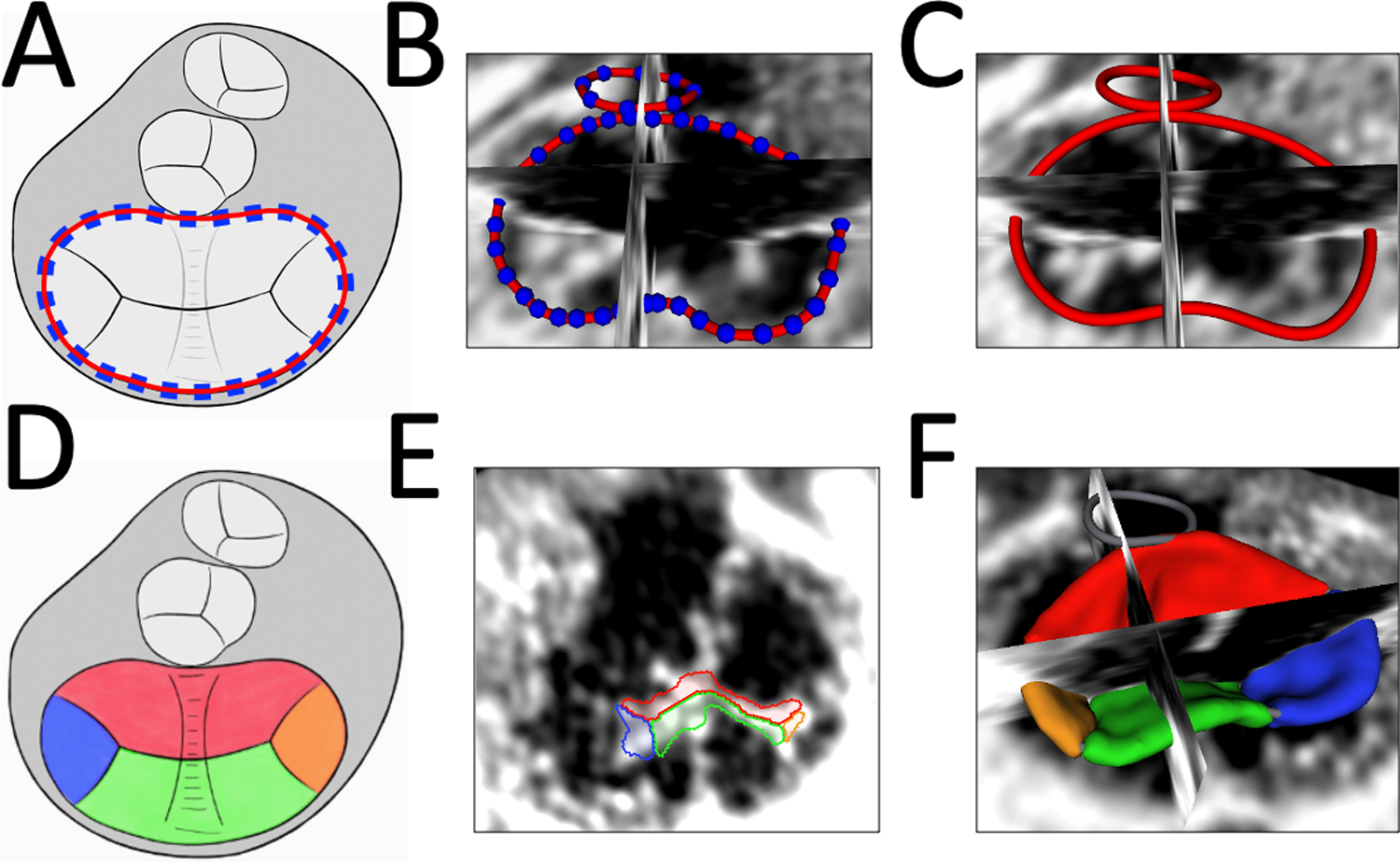
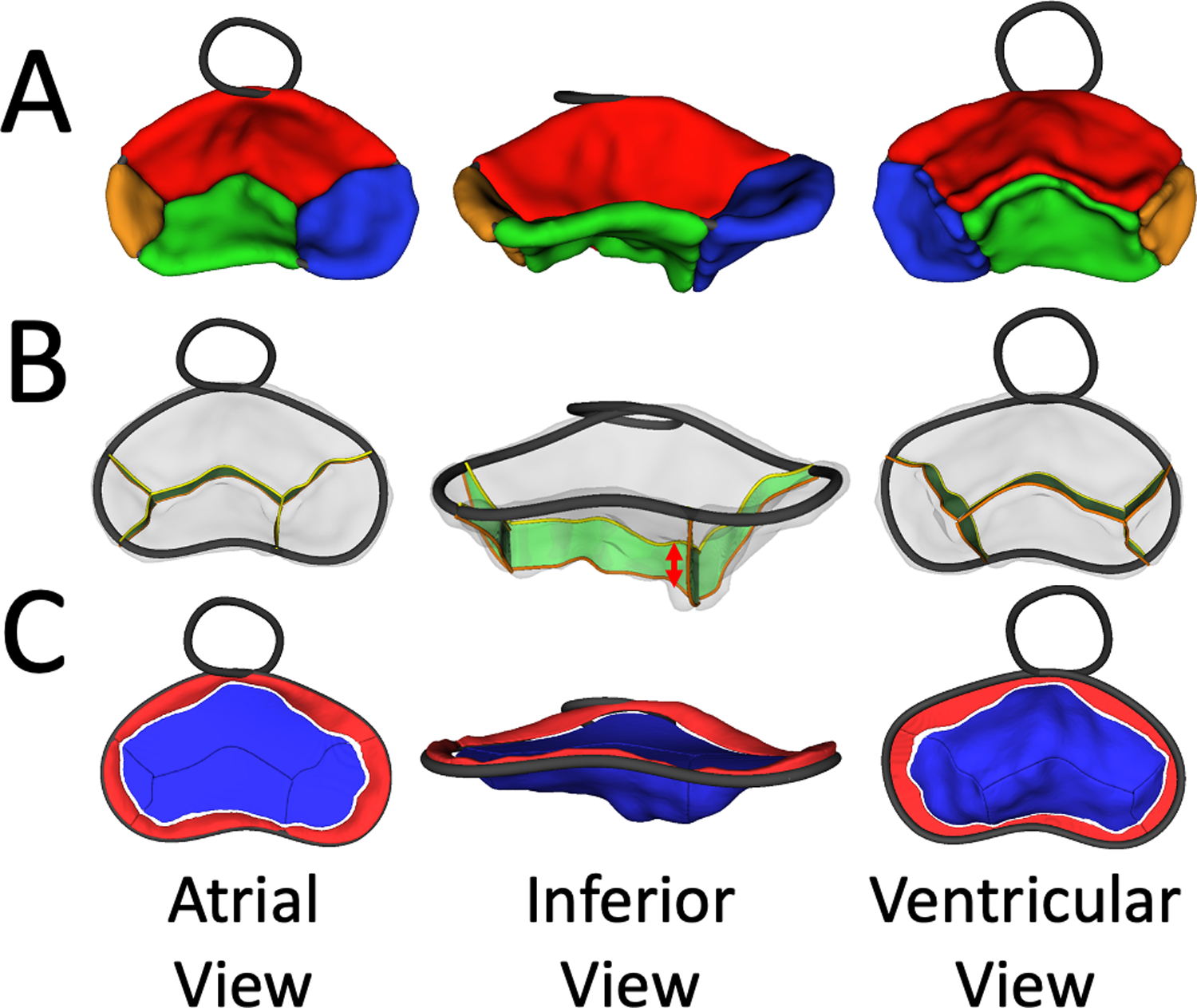
Methods: Novel open-source work flows were created in SlicerHeart for the modeling and quantification of CAVC valves on the basis of 3D echocardiographic images. These methods were applied to model the annulus, leaflets, and papillary muscle (PM) structure of 35 patients (29 with trisomy 21) with CAVC using transthoracic 3D echocardiography. The mean leaflet and annular shapes were calculated and visualized using shape analysis. Metrics of the complete native CAVC valve structure were compared with those of normal mitral valves using the Mann-Whitney U test. Associations between CAVC structure and atrioventricular valve regurgitation were analyzed.
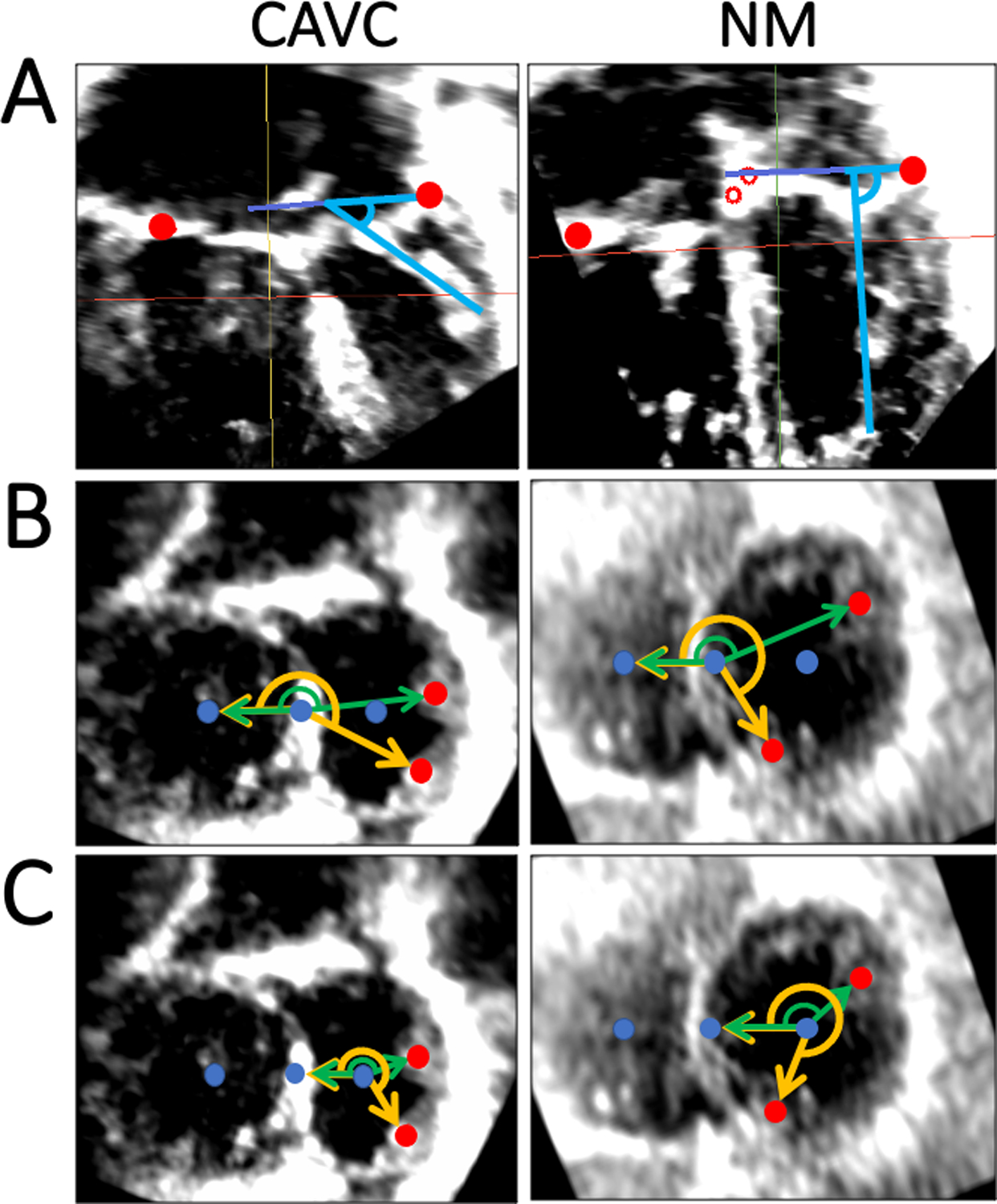
Results: CAVC leaflet metrics varied throughout systole. Compared with normal mitral valves, the left CAVC PMs were more acutely angled in relation to the annular plane (P < .001). In addition, the anterolateral PM was laterally and inferiorly rotated in CAVC, while the posteromedial PM was more superiorly and laterally rotated, relative to normal mitral valves (P < .001). Lower native CAVC atrioventricular valve annular height and annular height-to-valve width ratio before repair were both associated with moderate or greater left atrioventricular valve regurgitation after repair (P < .01).
Conclusions: It is feasible to model and quantify 3D CAVC structure using 3D echocardiographic images. The results demonstrate significant variation in CAVC structure across the cohort and differences in annular, leaflet, and PM structure compared with the mitral valve. These tools may be used in future studies to catalyze future research intended to identify structural associations of valve dysfunction and to optimize repair in this vulnerable and complex population.
Keywords: Congenital heart disease; Echocardiography; Valvular heart disease.
Copyright © 2022 American Society of Echocardiography. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Prifti E, Bonacchi M, Baboci A, Giunti G, Krakulli K, Vanini V. Surgical outcome of reoperation due to left atrioventricular valve regurgitation after previous correction of complete atrioventricular septal defect. J Card Surg. 2013;28:756–63. - PubMed
-
- Stulak JM, Burkhart HM, Dearani JA, Schaff HV, Cetta F, Barnes RD, et al. Reoperations after initial repair of complete atrioventricular septal defect. Ann Thorac Surg. 2009;87:1872–7; discussion 7–8. - PubMed
-
- Suzuki K, Tatsuno K, Kikuchi T, Mimori S. Predisposing factors of valve regurgitation in complete atrioventricular septal defect. J Am Coll Cardiol. 1998;32:1449–53. - PubMed
-
- Ten Harkel AD, Cromme-Dijkhuis AH, Heinerman BC, Hop WC, Bogers AJ. Development of left atrioventricular valve regurgitation after correction of atrioventricular septal defect. Ann Thorac Surg. 2005;79:607–12. - PubMed
-
- Mahmood F, Matyal R. A quantitative approach to the intraoperative echocardiographic assessment of the mitral valve for repair. Anesth Analg. 2015;121:34–58. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
