

Health insurance coverage in low-income and middle-income countries: progress made to date and related changes in private and public health expenditure
- PMID: 35537761
- PMCID: PMC9092126
- DOI: 10.1136/bmjgh-2022-008722
Health insurance coverage in low-income and middle-income countries: progress made to date and related changes in private and public health expenditure
Abstract
Introduction: Several low-income and middle-income countries (LMICs) have implemented health insurance programmes to foster accessibility to healthcare and reduce catastrophic household health expenditure. However, there is little information regarding the population coverage of health insurance schemes in LMICs and on the relationship between coverage and health expenditure. This study used open-access data to assess the level of health insurance coverage in LMICs and its relationship with health expenditure.
Methods: We searched for health insurance data for all LMICs and combined this with health expenditure data. We used descriptive statistics to explore levels of and trends in health insurance coverage over time. We then used linear regression models to investigate the relationship between health insurance coverage and sources of health expenditure and catastrophic household health expenditure.
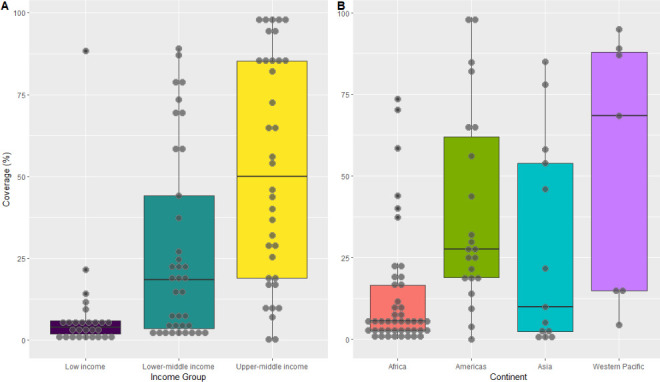
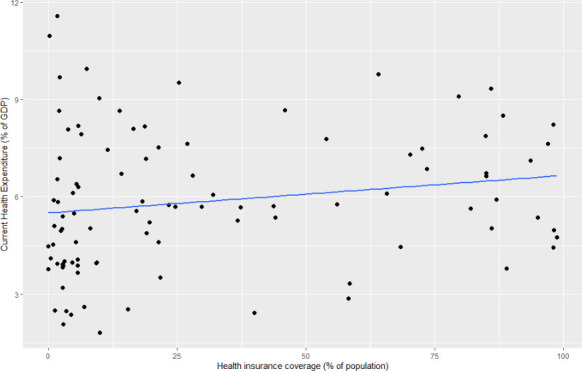
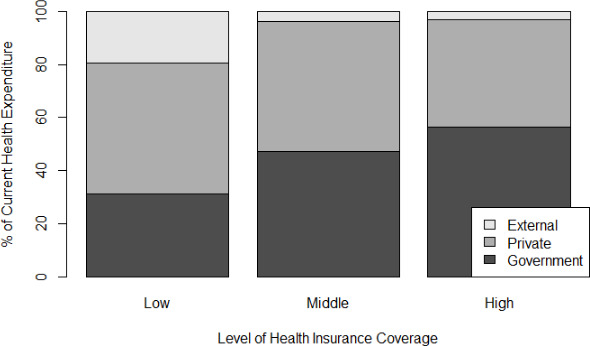
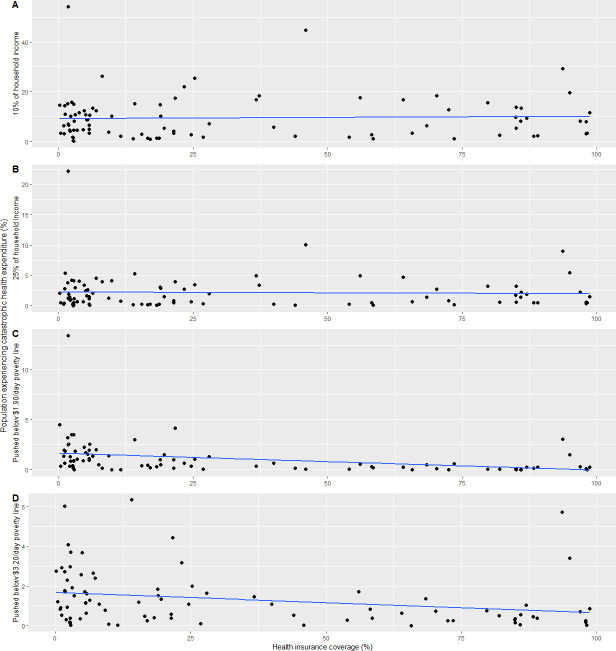
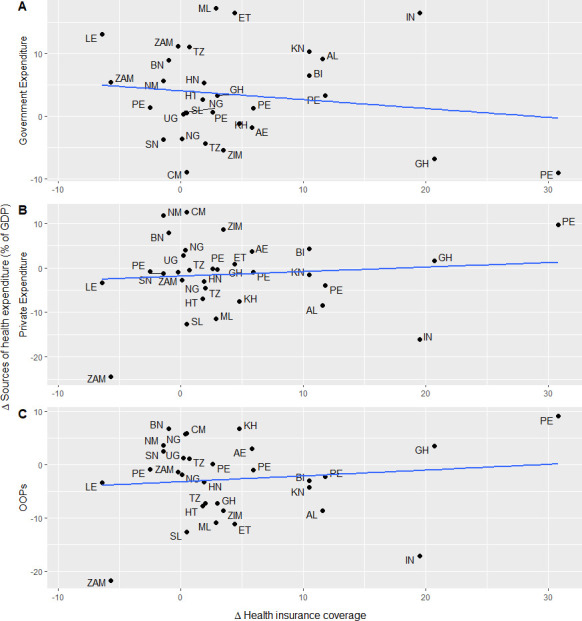
Results: We found health insurance data for 100 LMICs and combined this with overall health expenditure data for 99 countries and household health expenditure data for 89 countries. Mean health insurance coverage was 31.1% (range: 0%-98.7%), with wide variations across country-income groups. Average health insurance coverage was 7.9% in low-income countries, 27.3% in lower middle-income countries and 52.5% in upper middle-income countries. We did not find any association between health insurance coverage and health expenditure overall, though coverage was positively associated with public health spending. Additionally, health insurance coverage was not associated with levels of or reductions in catastrophic household health expenditure or impoverishment due to health expenditure.
Conclusion: These findings indicate that LMICs continue to have low levels of health insurance coverage and that health insurance may not necessarily reduce household health expenditure. However, the lack of regular estimates of health insurance coverage in LMICs does not allow us to draw solid conclusions on the relationship between health insurance coverage and health expenditure.
Keywords: Health economics; Health insurance; Health systems.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- WHO . World health report 2013: research for universal health coverage. Geneva: World Health Organization, 2013.
-
- Transforming our world: the 2030 agenda for sustainable development. GA Res A/70/L1, United nations 2015.
-
- World Health O, Carrin G, James C. Achieving universal health coverage: developing financing system. Geneva: World Health Organization, 2005.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources