

Adverse effects of COVID-19 mRNA vaccines: the spike hypothesis
- PMID: 35537987
- PMCID: PMC9021367
- DOI: 10.1016/j.molmed.2022.04.007
Adverse effects of COVID-19 mRNA vaccines: the spike hypothesis
Abstract
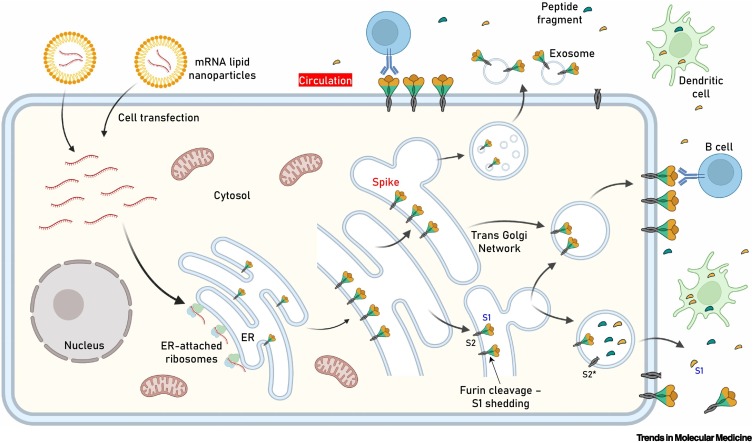
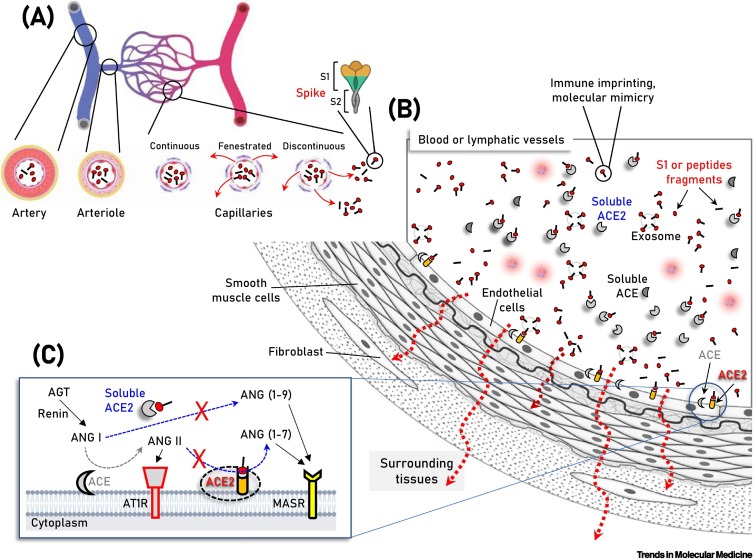
Vaccination is a major tool for mitigating the coronavirus disease 2019 (COVID-19) pandemic, and mRNA vaccines are central to the ongoing vaccination campaign that is undoubtedly saving thousands of lives. However, adverse effects (AEs) following vaccination have been noted which may relate to a proinflammatory action of the lipid nanoparticles used or the delivered mRNA (i.e., the vaccine formulation), as well as to the unique nature, expression pattern, binding profile, and proinflammatory effects of the produced antigens - spike (S) protein and/or its subunits/peptide fragments - in human tissues or organs. Current knowledge on this topic originates mostly from cell-based assays or from model organisms; further research on the cellular/molecular basis of the mRNA vaccine-induced AEs will therefore promise safety, maintain trust, and direct health policies.
Keywords: COVID-19; SARS-CoV-2; adverse effects; lipid nanoparticle; mRNA vaccine; spike protein.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
The spike hypothesis in vaccine-induced adverse effects: questions and answers.Trends Mol Med. 2022 Oct;28(10):797-799. doi: 10.1016/j.molmed.2022.07.009. Epub 2022 Sep 12. Trends Mol Med. 2022. PMID: 36114089 Free PMC article.
-
COVID-19 mRNA vaccine-induced adverse effects: unwinding the unknowns.Trends Mol Med. 2022 Oct;28(10):800-802. doi: 10.1016/j.molmed.2022.07.008. Epub 2022 Sep 12. Trends Mol Med. 2022. PMID: 36114090 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
