

Spatial and temporal fluctuations in COVID-19 fatality rates in Brazilian hospitals
- PMID: 35538260
- PMCID: PMC9307484
- DOI: 10.1038/s41591-022-01807-1
Spatial and temporal fluctuations in COVID-19 fatality rates in Brazilian hospitals
Erratum in
-
Author Correction: Spatial and temporal fluctuations in COVID-19 fatality rates in Brazilian hospitals.Nat Med. 2022 Jul;28(7):1509. doi: 10.1038/s41591-022-01939-4. Nat Med. 2022. PMID: 35835884 Free PMC article. No abstract available.
Abstract
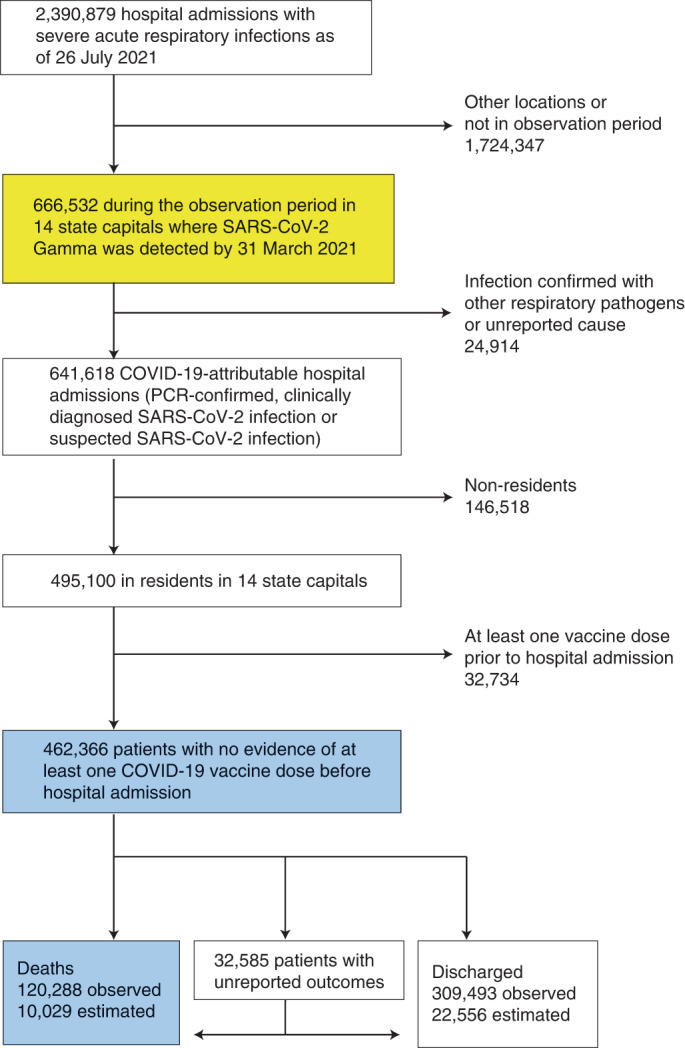
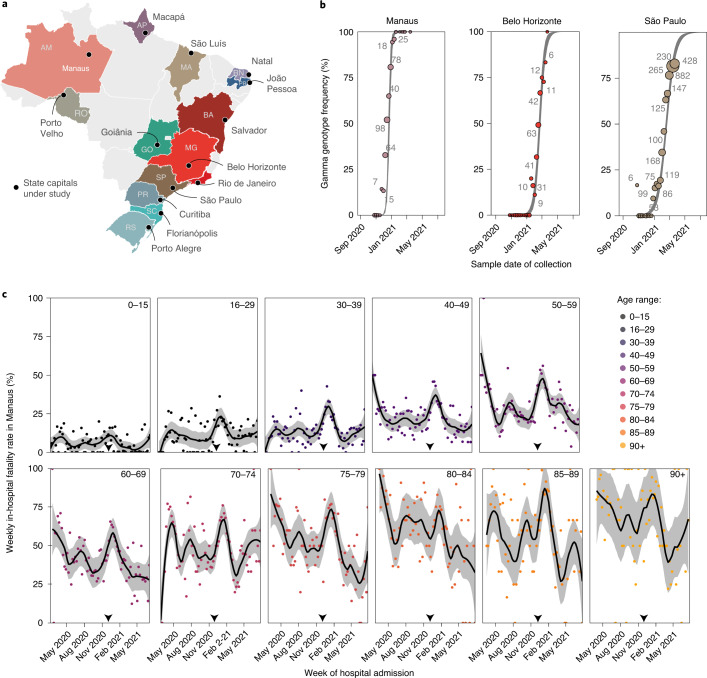
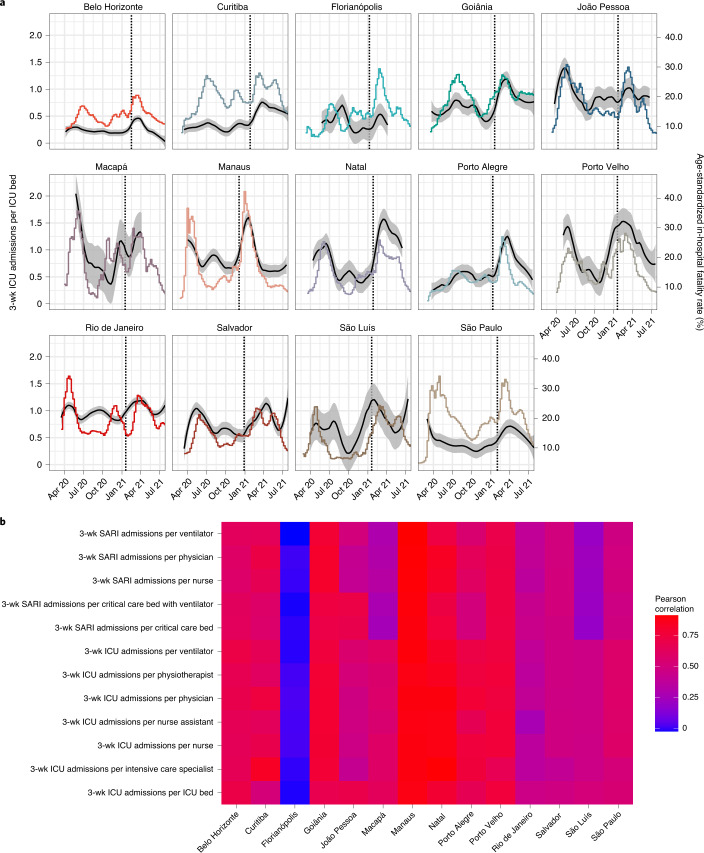
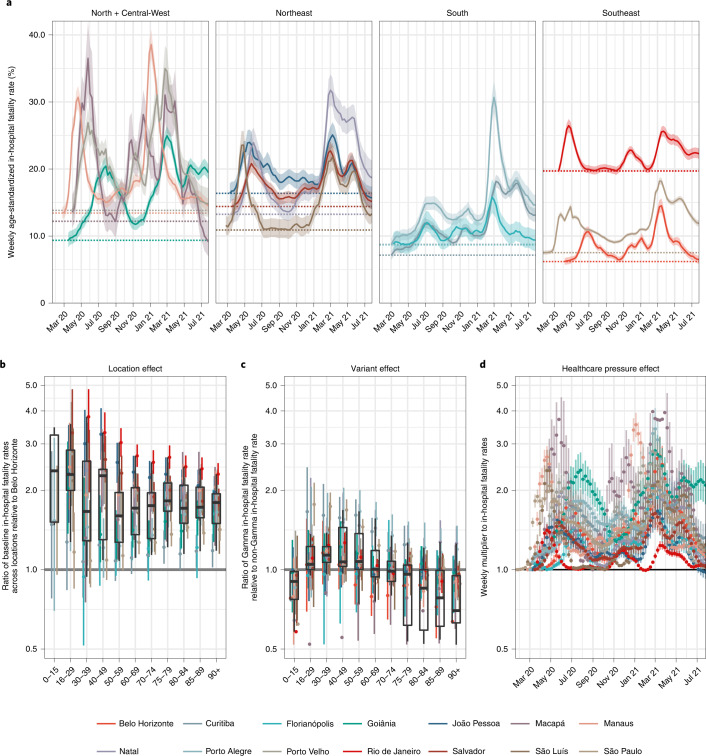
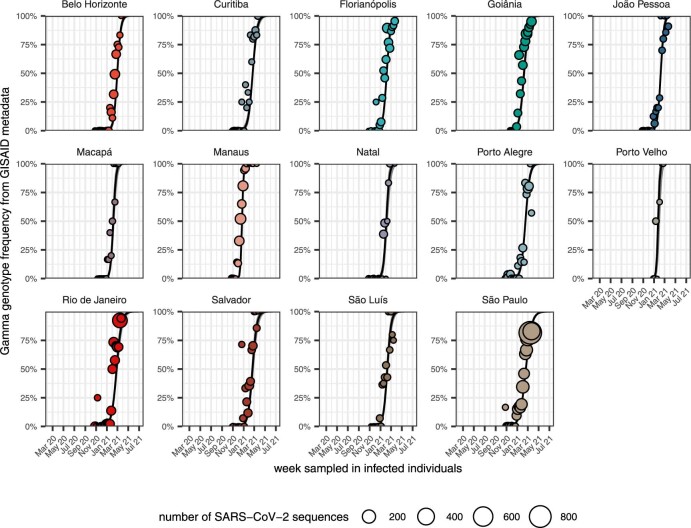
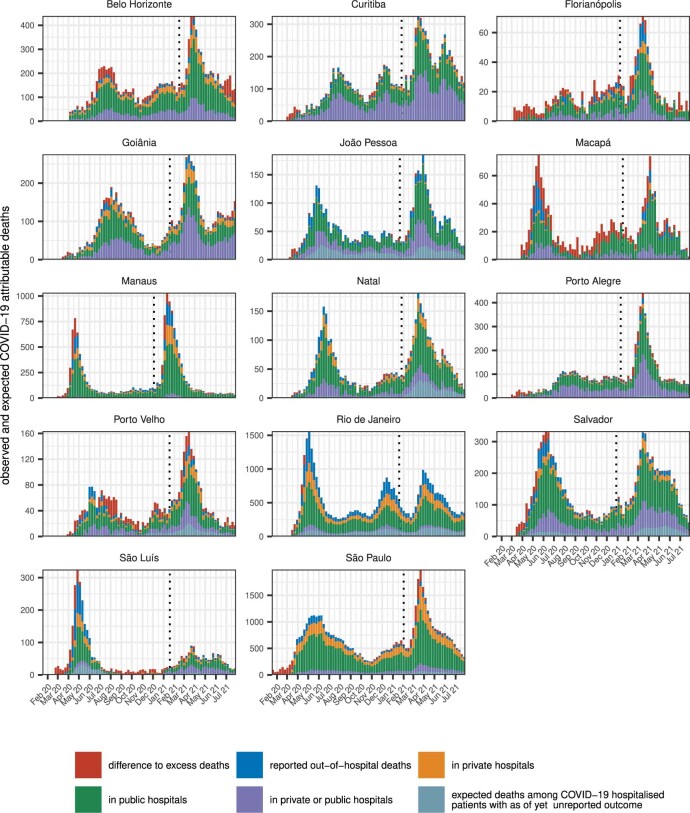
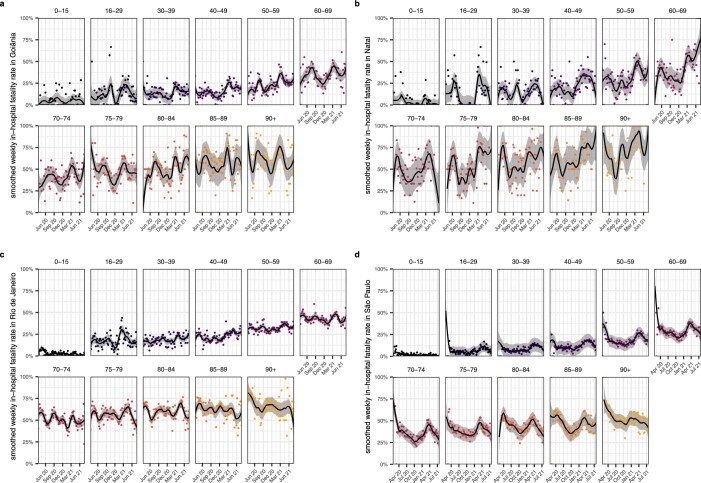
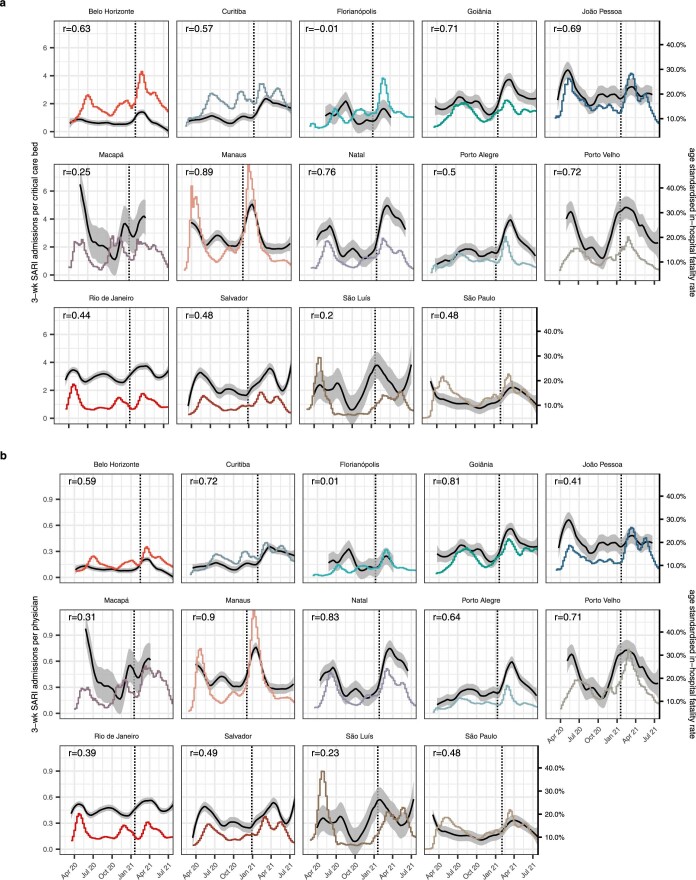
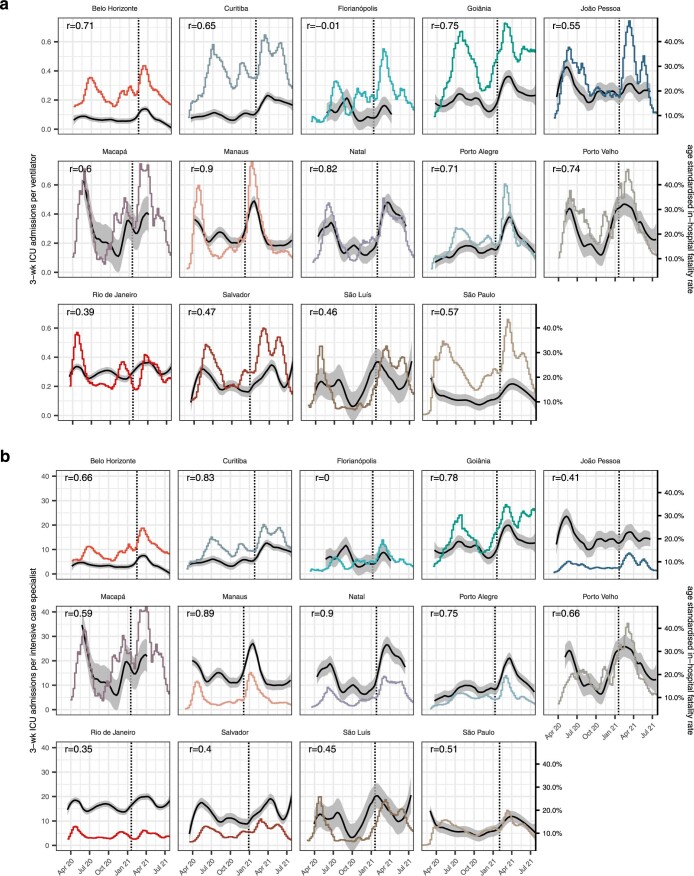
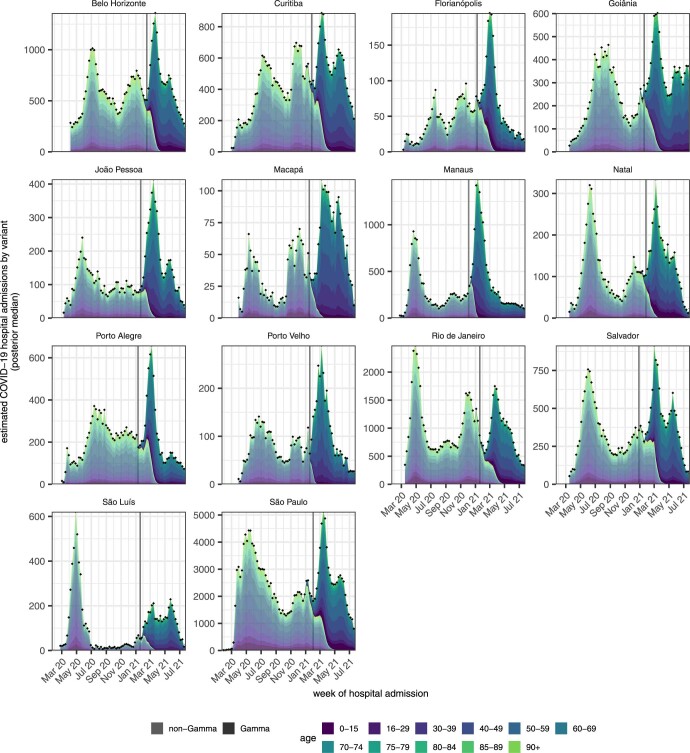
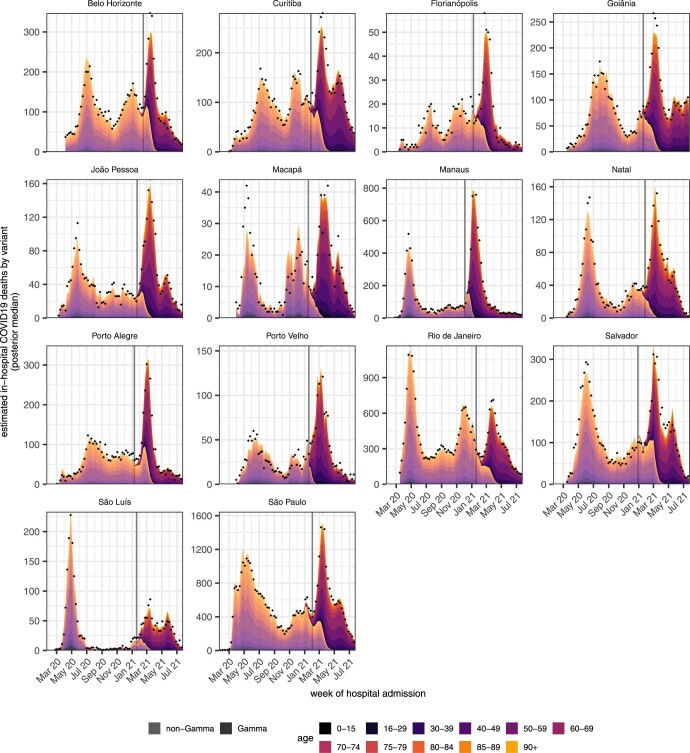
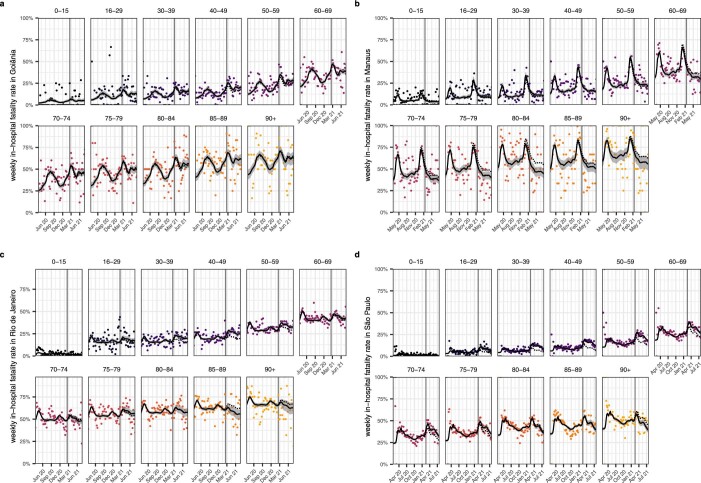
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Gamma variant of concern has spread rapidly across Brazil since late 2020, causing substantial infection and death waves. Here we used individual-level patient records after hospitalization with suspected or confirmed coronavirus disease 2019 (COVID-19) between 20 January 2020 and 26 July 2021 to document temporary, sweeping shocks in hospital fatality rates that followed the spread of Gamma across 14 state capitals, during which typically more than half of hospitalized patients aged 70 years and older died. We show that such extensive shocks in COVID-19 in-hospital fatality rates also existed before the detection of Gamma. Using a Bayesian fatality rate model, we found that the geographic and temporal fluctuations in Brazil's COVID-19 in-hospital fatality rates were primarily associated with geographic inequities and shortages in healthcare capacity. We estimate that approximately half of the COVID-19 deaths in hospitals in the 14 cities could have been avoided without pre-pandemic geographic inequities and without pandemic healthcare pressure. Our results suggest that investments in healthcare resources, healthcare optimization and pandemic preparedness are critical to minimize population-wide mortality and morbidity caused by highly transmissible and deadly pathogens such as SARS-CoV-2, especially in low- and middle-income countries.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
Report 46: Factors driving extensive spatial and temporal fluctuations in COVID-19 fatality rates in Brazilian hospitals.medRxiv [Preprint]. 2021 Nov 2:2021.11.01.21265731. doi: 10.1101/2021.11.01.21265731. medRxiv. 2021. Update in: Nat Med. 2022 Jul;28(7):1476-1485. doi: 10.1038/s41591-022-01807-1. PMID: 34751273 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
