

Acute myocardial infarction with simultaneous total occlusion of the left anterior descending artery and right coronary artery successfully treated with percutaneous coronary intervention
- PMID: 35538416
- PMCID: PMC9088105
- DOI: 10.1186/s12872-022-02652-3
Acute myocardial infarction with simultaneous total occlusion of the left anterior descending artery and right coronary artery successfully treated with percutaneous coronary intervention
Abstract
Background: Simultaneous thrombosis in more than one coronary artery is an uncommon angiographic finding in patients with acute ST-segment elevation myocardial infarction. It is difficult to identify using 12-lead electrocardiography and usually leads to cardiogenic shock and fatal outcomes, including sudden cardiac death. Therefore, immediate revascularization and adequate mechanical circulatory support are required.
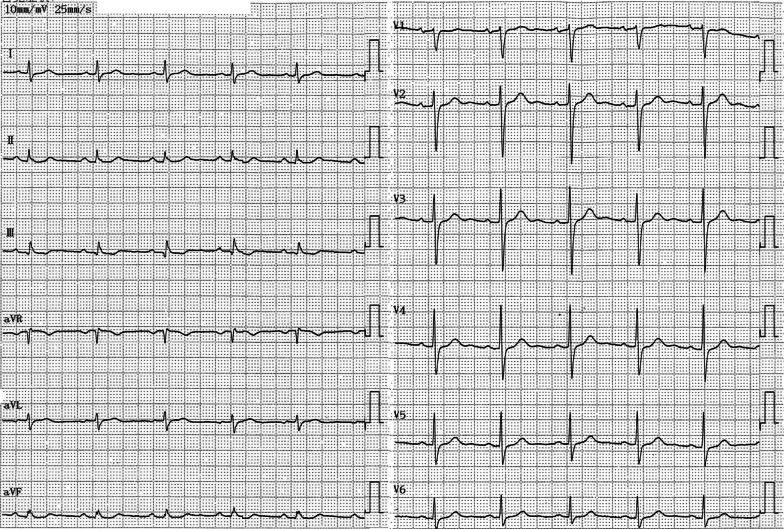
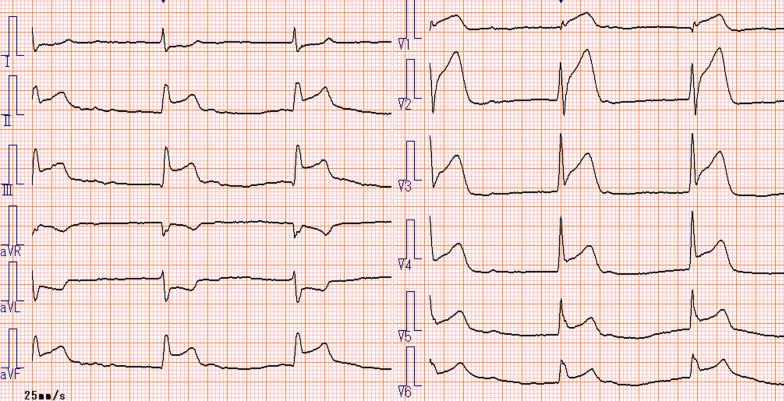
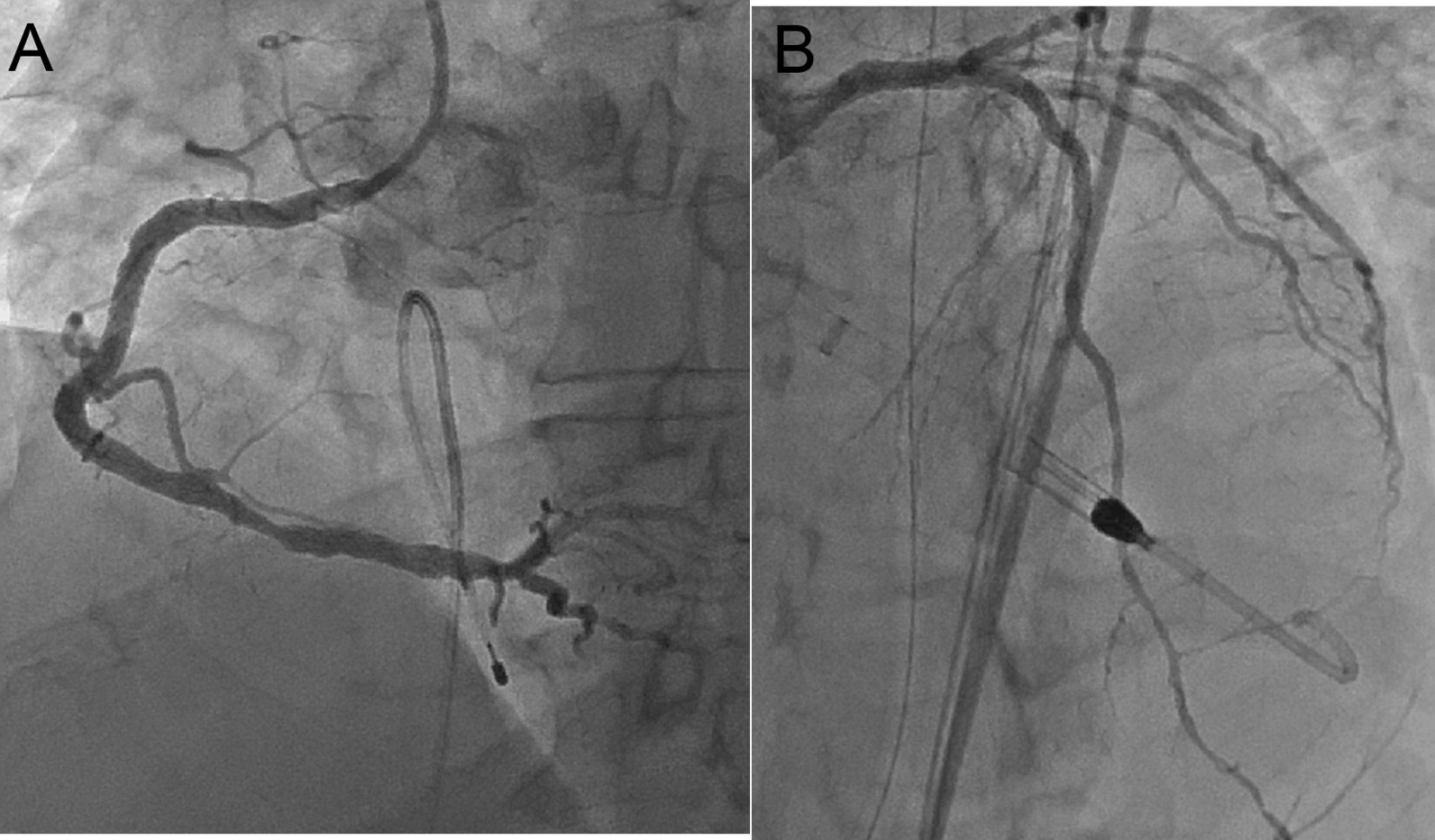
Case presentation: We report the case of a 58-year-old man who presented with vomiting and chest pain complicated by cardiogenic shock and complete atrioventricular block. Electrocardiography revealed ST-segment elevation in leads II, III, aVF, and V1-V6. Emergency coronary angiography revealed total occlusion of the proximal left anterior descending artery and right coronary artery. The patient successfully underwent primary percutaneous coronary intervention with ballooning and stenting for both arteries. An Impella CP was inserted during the procedure. Fifty-seven days after admission, he had New York Heart Association class II heart failure and was transferred to a rehabilitation hospital.
Conclusions: Acute double-vessel coronary thrombosis, a serious event with a high mortality rate, requires prompt diagnosis and management to prevent complications such as cardiogenic shock and ventricular arrhythmias. A combination of judicious medical treatment, efficient primary percutaneous coronary intervention, and early mechanical support device insertion is crucial to improve the survival rate of patients with this disease.
Keywords: Acute myocardial infarction; Impella CP; Simultaneous total occlusion.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





Similar articles
-
Double coronary artery thrombosis presenting as acute extensive anterior ST-segment elevation myocardial infarction.J Chin Med Assoc. 2013 Jul;76(7):407-10. doi: 10.1016/j.jcma.2013.03.007. Epub 2013 May 9. J Chin Med Assoc. 2013. PMID: 23664732
-
Multiple coronary artery thrombosis in a 41-year-old male patient presenting with ST-segment elevation myocardial infarction.J Invasive Cardiol. 2012 Mar;24(3):E43-6. J Invasive Cardiol. 2012. PMID: 22388313
-
Emergency coronary stenting for complete thrombotic occlusion of an unprotected left main coronary artery in acute myocardial infarction complicated by cardiogenic shock in an octogenarian patient--a case report.Angiology. 2002 Jan-Feb;53(1):95-8. doi: 10.1177/000331970205300113. Angiology. 2002. PMID: 11865840
-
A Suspected Case of Acute Embolic Myocardial Infarction Following Direct-Current Cardioversion of Atrial Fibrillation.Am J Case Rep. 2018 Nov 2;19:1306-1310. doi: 10.12659/AJCR.911469. Am J Case Rep. 2018. PMID: 30385736 Free PMC article. Review.
-
Culprit Vessel-Only Versus Multivessel Percutaneous Coronary Intervention in Patients With Cardiogenic Shock Complicating ST-Segment-Elevation Myocardial Infarction: A Collaborative Meta-Analysis.Circ Cardiovasc Interv. 2017 Nov;10(11):e005582. doi: 10.1161/CIRCINTERVENTIONS.117.005582. Circ Cardiovasc Interv. 2017. PMID: 29146672 Review.
Cited by
-
A STEMI Complicated by Cardiogenic Shock Due to Simultaneous Acute Thrombosis of Two Coronary Vessels in the 'Deadly Double Infarct Syndrome': A Case Report and Discussion of Literature.J Clin Med. 2024 Dec 10;13(24):7511. doi: 10.3390/jcm13247511. J Clin Med. 2024. PMID: 39768439 Free PMC article.
-
The effect of extent and localization of precordial ST-segment depression in acute inferior myocardial infarction as an indicator of infarct severity, coronary artery involvement, and cardiac outcomes.Ther Adv Cardiovasc Dis. 2025 Jan-Dec;19:17539447251326154. doi: 10.1177/17539447251326154. Epub 2025 Mar 14. Ther Adv Cardiovasc Dis. 2025. PMID: 40084462 Free PMC article.
References
-
- Maagh P, Wickenbrock I, Schrage MO, Trappe HJ, Meissner A. Acute simultaneous proximal occlusion of two major coronary arteries in acute myocardial infarction: Successful treatment with percutaneous coronary intervention. J Interv Cardiol. 2008;21:483–492. doi: 10.1111/j.1540-8183.2008.00394.x. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
