

Survival and predictors of asphyxia among neonates admitted in neonatal intensive care units of public hospitals of Addis Ababa, Ethiopia, 2021: a retrospective follow-up study
- PMID: 35538451
- PMCID: PMC9087963
- DOI: 10.1186/s12887-022-03238-w
Survival and predictors of asphyxia among neonates admitted in neonatal intensive care units of public hospitals of Addis Ababa, Ethiopia, 2021: a retrospective follow-up study
Abstract
Background: Globally, perinatal asphyxia (PNA) is a significant cause of most neonatal deaths. Similarly, the burden of birth asphyxia in Ethiopia remains high (22.52%) and has been noted the second leading cause of neonatal mortality. Thus, researches on survival status and predictors of perinatal asphyxia are critical to tackle it. Therefore, the current study intended to determine the survival status and predictors of asphyxia among neonates admitted in Neonatal Intensive Care Units of public hospitals, Addis Ababa, Ethiopia.
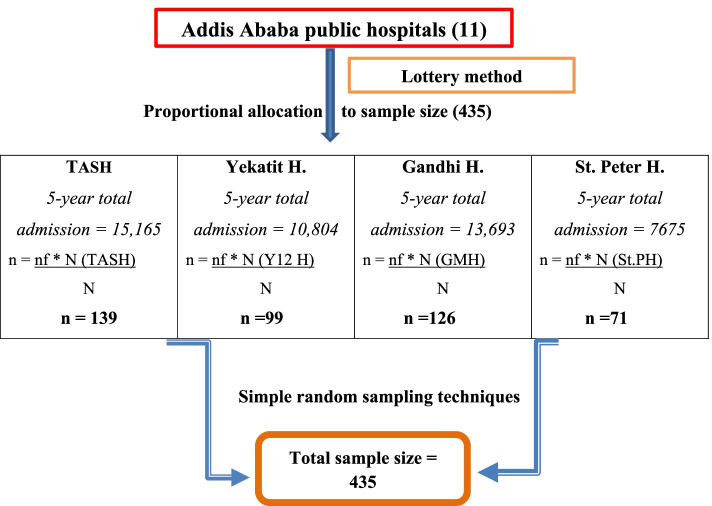
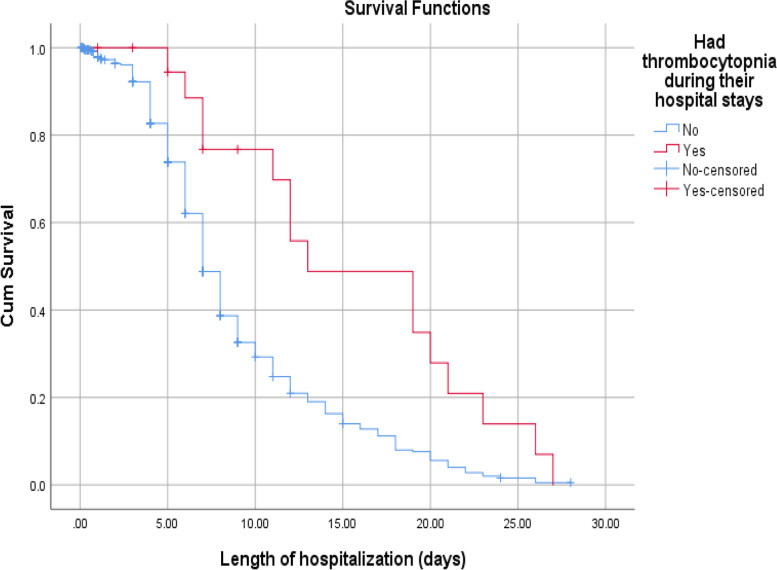
Methods: Hospital-based retrospective follow-up study was conducted in four selected public hospitals of Addis Ababa from January 2016 to December 2020. Data were collected using a pretested structured questionnaire. Epi-data 4.6 and STATA Version 16 was used for data entry and analysis, respectively. Kaplan-Meier survival curve, log-rank test and Median time were computed. To find the predictors of time to recovery, a multivariable Cox proportional hazards regression model was fitted, and variables with a P-value less than 0.05 were considered statistically significant. Finally, the Schoenfeld residual test was used to check overall model fitness.
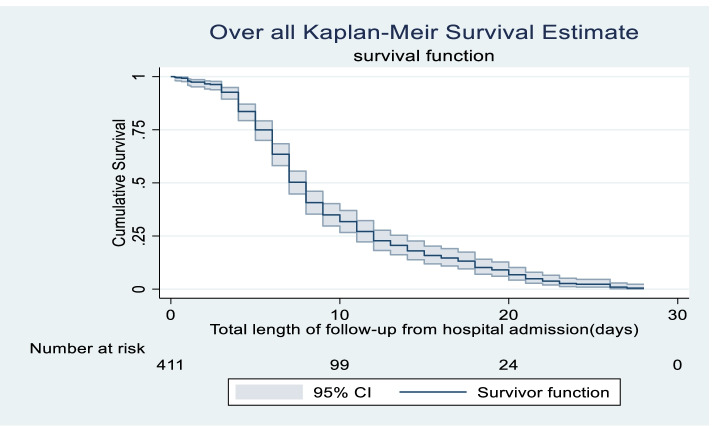
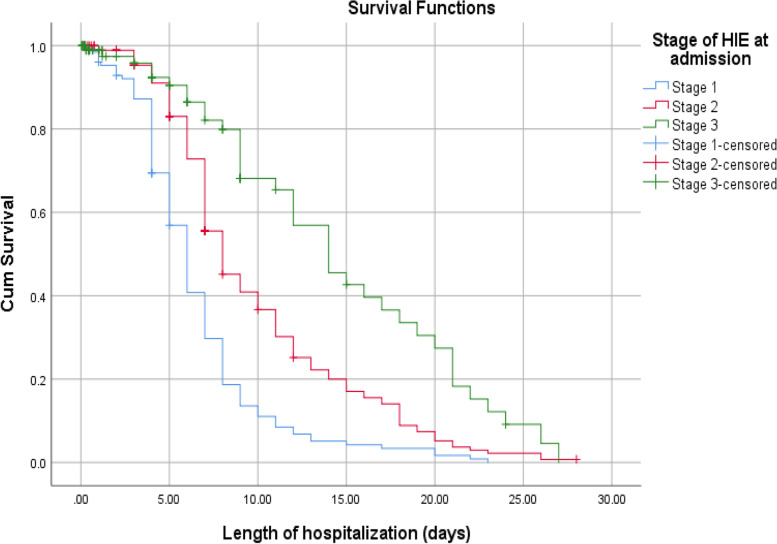
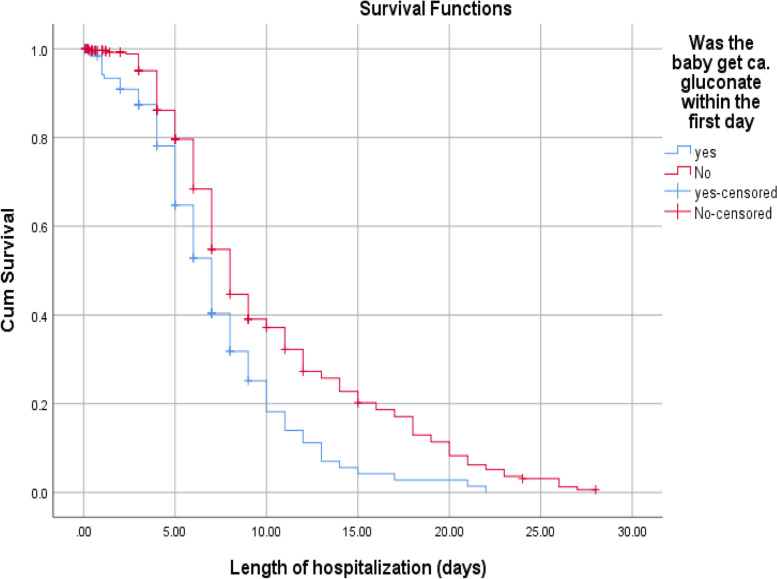
Result: Four hundred eleven admitted asphyxiated babies were followed a total of 3062 neonate-days with a minimum of 1 h to a maximum of 28 days. The Overall incidence density rate of survival was 10 (95% CI: 0.08-0.11) per 100 neonate-days of observation with a median recovery time of 8 days (95% CI: 7.527-8.473). Low birth weight (Adjusted hazard ratio [AHR]: 0.67, 95% CI: 0.47-0.96), stage II hypoxic ischemic encephalopathy (HIE) (AHR: 0.70, 95% CI: 0.51-0.97), stage III HIE (AHR: 0.44, 95% CI: 0.27-0.71), seizure (AHR: 0.61, 95% CI: 0.38-0.97), thrombocytopenia (AHR: 0.44, 95% CI: 0.24-0.80) and calcium gluconate (AHR: 0.75, 95% CI: 0.58-0.99) were found to be independent predictors of time to recovery of asphyxiated neonates.
Conclusion: In the current findings, the recovery time was prolonged compared to others finding. This implies early prevention, strict monitoring and taking appropriate measures timely is mandatory before babies transferred into highest stage of HIE and managing complications are recommended to hasten recovery time and increase survival of neonates.
Keywords: Median recovery time; Perinatal-asphyxia; Predictors; Survival-status.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Kliegman R, ST. Geme J, Stanton B, Schor N. Nelson textbook of PEDIATRICS. 21th Edition. 2020. pp. 3944–60.
-
- Padayachee N, Ballot DE. Outcomes of neonates with perinatal asphyxia at a tertiary academic hospital in Johannesburg, South Africa. SAJCH South African J Child Heal. 2013;7(3):93.
-
- Gillam-krakauer MGJC. Birth Asphyxia. Br Med J. 2020;2:2.
MeSH terms
LinkOut - more resources
Full Text Sources
