

Surgical treatment of recurrent intussusception induced by intestinal lymphoid hyperplasia in a child: is bowel resection always necessary? A case report
- PMID: 35538469
- PMCID: PMC9092808
- DOI: 10.1186/s12893-022-01608-w
Surgical treatment of recurrent intussusception induced by intestinal lymphoid hyperplasia in a child: is bowel resection always necessary? A case report
Abstract
Background: Intussusception recurrence (IR) induced by intestinal lymphoid hyperplasia (ILH) in children is rare, and surgical treatment is the final resort if IR is refractory to medications and non-surgical interventions. To date, only a few case reports have described surgical management of ILH-induced IR in children, all involving bowel resection regardless of whether there are bowel necrosis and perforation.
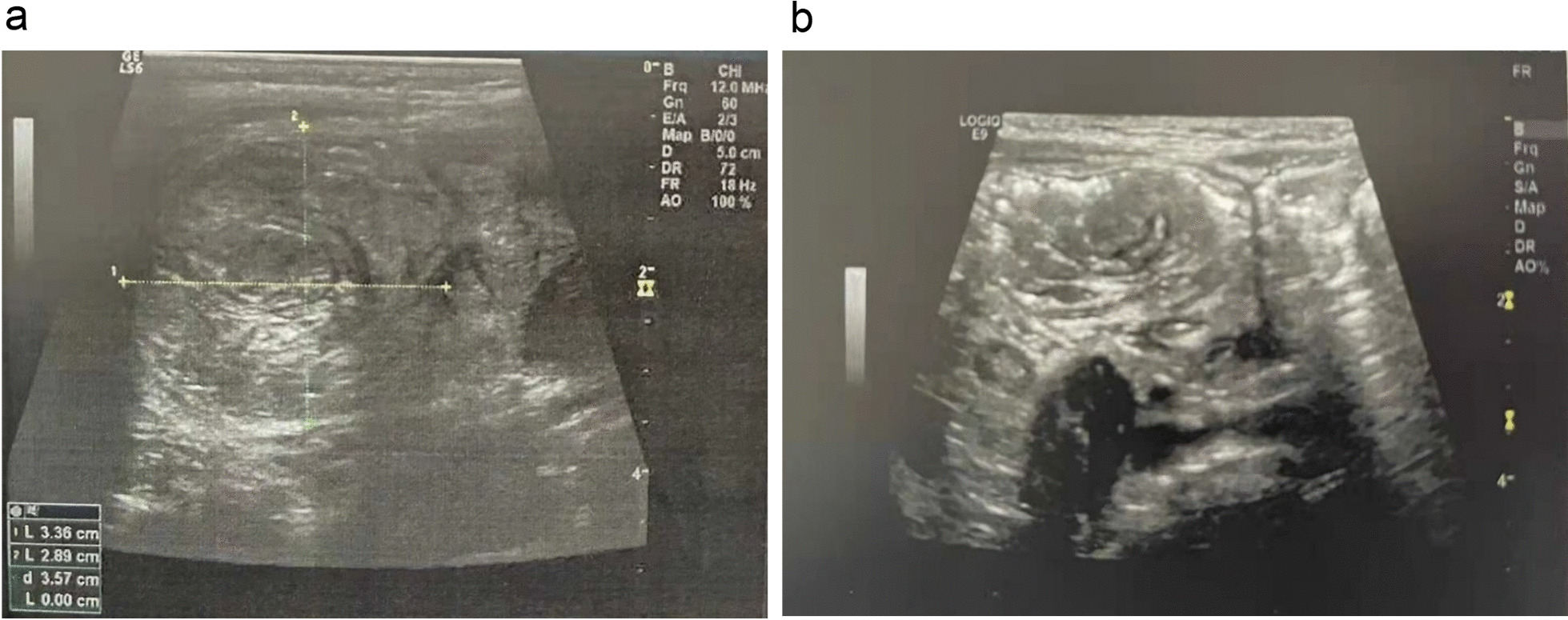
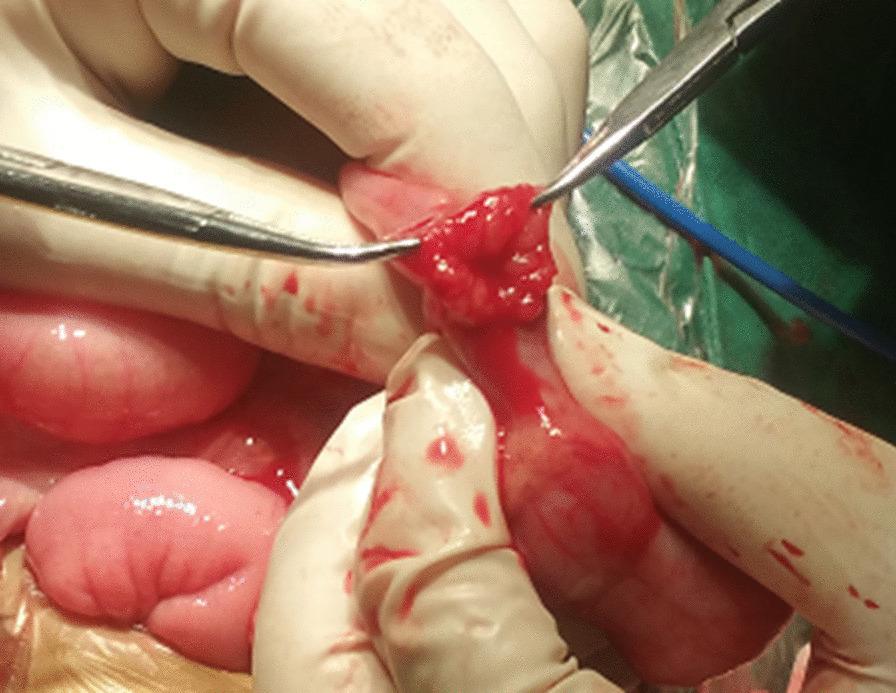
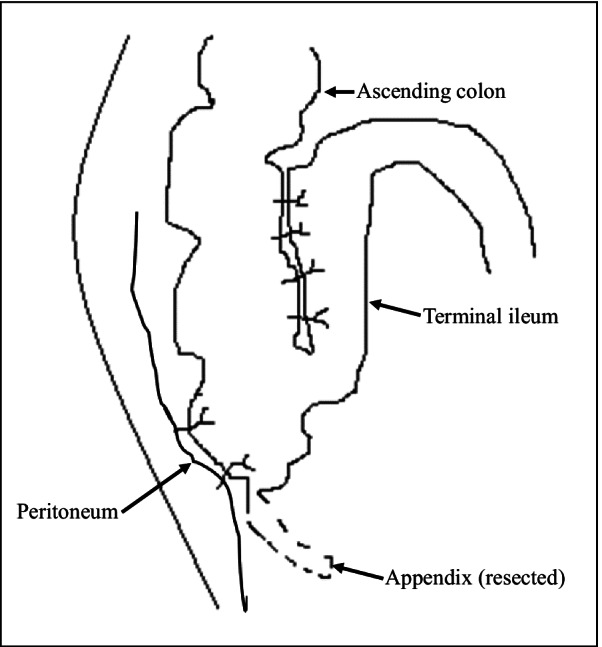
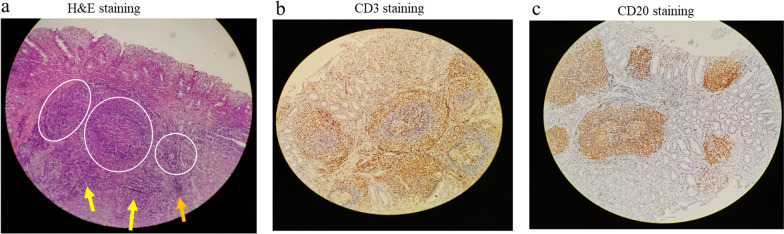
Case presentation: A 2-year-old boy was transferred to our department due to IR. His main complaint was abdominal pain. Color Doppler ultrasound confirmed ileocecal intussusception while no other abnormalities were found. A final diagnosis of IR with unknown causes was made. Repeated saline enema reductions and dexamethasone failed to cure the IR. Laparotomy was eventually performed after almost 10 episodes of IR. Intraoperatively, distal ileum thickening with palpable masses without bowel necrosis and perforation was noted. ILH was suspected and a biopsy of the affected intestine was performed. Histopathological analysis confirmed ILH. The intussusception was manually reduced, the terminal ileum and the ileocecal junction were fixed to the paralleled ascending colon and the posterior peritoneum respectively, and no bowel resection was performed. The postoperative recovery was uneventful and no IR was observed during over 5 years of follow-up.
Conclusions: As far as we are aware, this is the first report of successful surgical treatment of ILH-induced pediatric IR without bowel resection in a child. Our experience suggests bowel resection may be unnecessary if bowel necrosis and perforation are absent.
Keywords: Bowel resection; Case report; Enema reduction; Intestinal lymphoid hyperplasia; Intussusception recurrence.
© 2022. The Author(s).
Conflict of interest statement
The authors have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
