

Effects of preoperative high-oral protein loading on short- and long-term renal outcomes following cardiac surgery: a cohort study
- PMID: 35538495
- PMCID: PMC9092825
- DOI: 10.1186/s12967-022-03410-x
Effects of preoperative high-oral protein loading on short- and long-term renal outcomes following cardiac surgery: a cohort study
Abstract
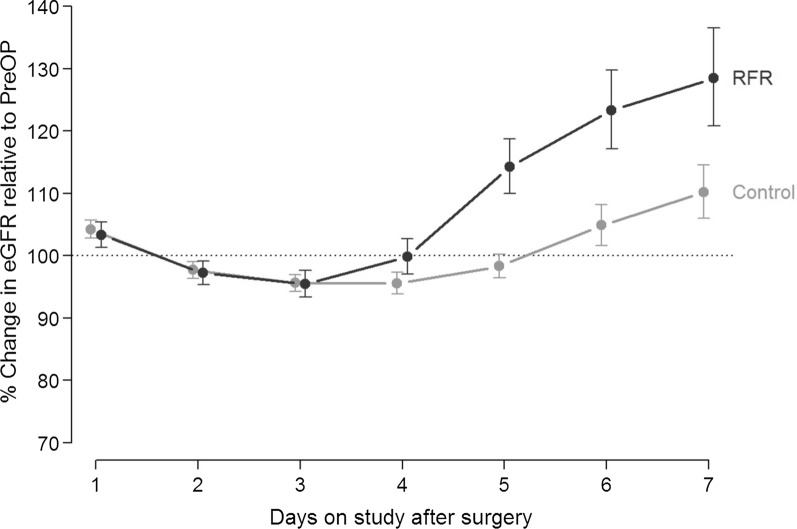
Background: Post-cardiac surgery acute kidney injury (AKI) is associated with increased mortality. A high-protein meal enhances the renal blood flow and glomerular filtration rate (GFR) and might protect the kidneys from acute ischemic insults. Hence, we assessed the effect of a preoperative high-oral protein load on post-cardiac surgery renal function and used experimental models to elucidate mechanisms by which protein might stimulate kidney-protective effects.
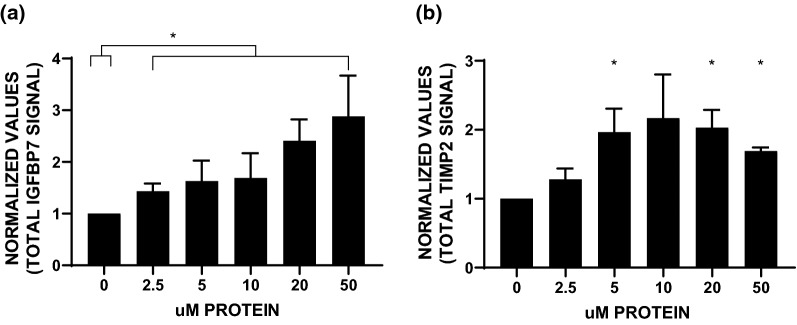
Methods: The prospective "Preoperative Renal Functional Reserve Predicts Risk of AKI after Cardiac Operation" study follow-up was extended to postoperative 12 months for 109 patients. A 1:2 ratio propensity score matching method was used to identify a control group (n = 214) to comparatively evaluate the effects of a preoperative protein load and standard care. The primary endpoints were AKI development and postoperative estimated GFR (eGFR) loss at 3 and 12 months. We also assessed the secretion of tissue inhibitor of metalloproteases-2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7), biomarkers implicated in mediating kidney-protective mechanisms in human kidney tubular cells that we exposed to varying protein concentrations.
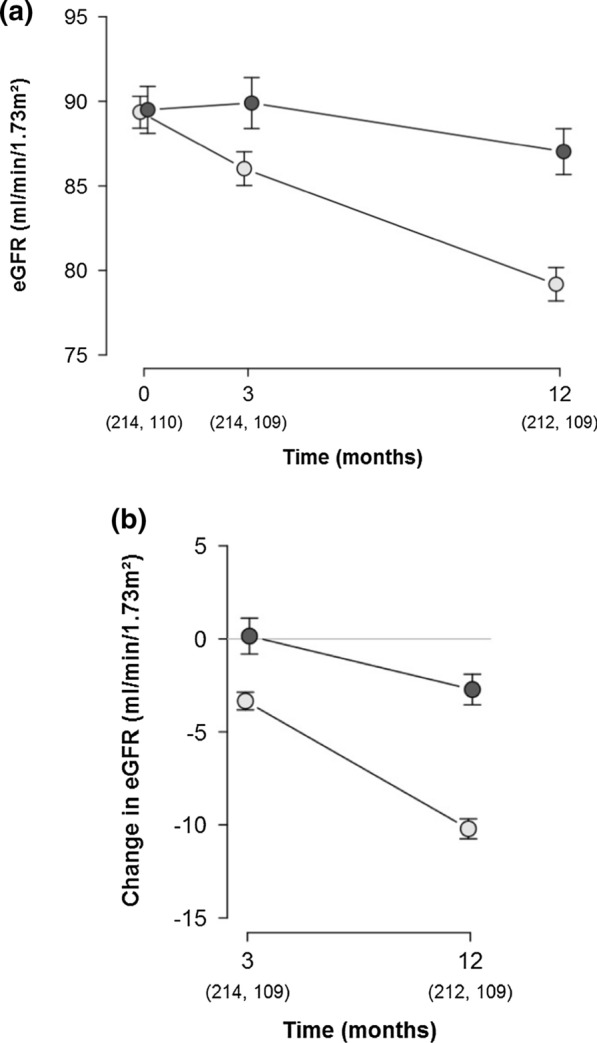
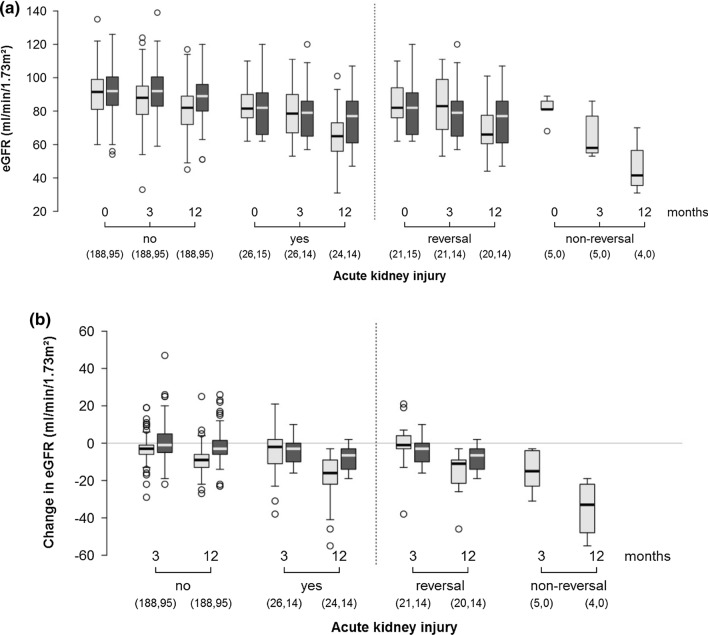
Results: The AKI rate did not differ between the protein loading and control groups (13.6 vs. 12.3%; p = 0.5). However, the mean eGFR loss was lower in the former after 3 months (0.1 [95% CI - 1.4, - 1.7] vs. - 3.3 [95% CI - 4.4, - 2.2] ml/min/1.73 m2) and 12 months (- 2.7 [95% CI - 4.2, - 1.2] vs - 10.2 [95% CI - 11.3, - 9.1] ml/min/1.73 m2; p < 0.001 for both). On stratification based on AKI development, the eGFR loss after 12 months was also found to be lower in the former (- 8.0 [95% CI - 14.1, - 1.9] vs. - 18.6 [95% CI - 23.3, - 14.0] ml/min/1.73 m2; p = 0.008). A dose-response analysis of the protein treatment of the primary human proximal and distal tubule epithelial cells in culture showed significantly increased IGFBP7 and TIMP-2 expression.
Conclusions: A preoperative high-oral protein load did not reduce AKI development but was associated with greater renal function preservation in patients with and without AKI at 12 months post-cardiac surgery. The potential mechanisms of action by which protein loading may induce a kidney-protective response might include cell cycle inhibition of renal tubular epithelial cells. Clinical trial registration ClinicalTrials.gov: NCT03102541 (retrospectively registered on April 5, 2017) and ClinicalTrials.gov: NCT03092947 (retrospectively registered on March 28, 2017).
Keywords: Acute kidney injury; Chronic kidney disease; Kidney stress test; Renal recovery.
© 2022. The Author(s).
Conflict of interest statement
KT has received speaking fees from Actelion and Bayer outside the submitted work. WS has received speaker/consultancy fees from Pfizer and Bayer Pharma AG outside the submitted work. JAK discloses inventorship on a patent application held by the Universities of Pittsburgh, and Munster, and Astute Medical (US2018/074054A1) for use of TIMP-2 and IGFBP7 in conjunction with interventions to protect the kidney. CR reports support for acting as an advisory board member for ASAHI, Baxter, GE, Jafron, and Medtronic, and speaker’s fees from Astute, bioMérieux, B. Braun, Cytosorbents, ESTOR, FMC, and Toray, all unrelated to the submitted work. All other authors have declared that no conflict of interests exists.
Figures
Similar articles
-
Persistent decrease of renal functional reserve in patients after cardiac surgery-associated acute kidney injury despite clinical recovery.Nephrol Dial Transplant. 2019 Feb 1;34(2):308-317. doi: 10.1093/ndt/gfy227. Nephrol Dial Transplant. 2019. PMID: 30053231
-
Preoperative Renal Functional Reserve Predicts Risk of Acute Kidney Injury After Cardiac Operation.Ann Thorac Surg. 2018 Apr;105(4):1094-1101. doi: 10.1016/j.athoracsur.2017.12.034. Epub 2018 Jan 31. Ann Thorac Surg. 2018. PMID: 29382510
-
Urine Biomarkers of Tubular Renal Cell Damage for the Prediction of Acute Kidney Injury After Cardiac Surgery-A Pilot Study.J Cardiothorac Vasc Anesth. 2017 Dec;31(6):2072-2079. doi: 10.1053/j.jvca.2017.04.024. Epub 2017 Apr 16. J Cardiothorac Vasc Anesth. 2017. PMID: 28803769
-
The Accuracy of Urinary TIMP-2 and IGFBP7 for the Diagnosis of Cardiac Surgery-Associated Acute Kidney Injury: A Systematic Review and Meta-Analysis.J Intensive Care Med. 2020 Oct;35(10):1013-1025. doi: 10.1177/0885066618807124. Epub 2018 Oct 30. J Intensive Care Med. 2020. PMID: 30376758
-
Predictive value of cell cycle arrest biomarkers for cardiac surgery-associated acute kidney injury: a meta-analysis.Br J Anaesth. 2018 Aug;121(2):350-357. doi: 10.1016/j.bja.2018.02.069. Epub 2018 May 3. Br J Anaesth. 2018. PMID: 30032873 Review.
Cited by
-
Recruitment of renal functional reserve by intravenous amino acid loading in a sheep model of cardiopulmonary bypass.Intensive Care Med Exp. 2025 Jul 10;13(1):71. doi: 10.1186/s40635-025-00774-4. Intensive Care Med Exp. 2025. PMID: 40637920 Free PMC article.
-
Cardiopulmonary bypass associated acute kidney injury: better understanding and better prevention.Ren Fail. 2024 Dec;46(1):2331062. doi: 10.1080/0886022X.2024.2331062. Epub 2024 Mar 21. Ren Fail. 2024. PMID: 38515271 Free PMC article. Review.
-
Postoperative 20% Albumin Infusion and Acute Kidney Injury in High-Risk Cardiac Surgery Patients: The ALBICS AKI Randomized Clinical Trial.JAMA Surg. 2025 Aug 1;160(8):835-844. doi: 10.1001/jamasurg.2025.1683. JAMA Surg. 2025. PMID: 40498523 Clinical Trial.
-
Dietary modifications affect renal recovery during the healing phase following ischemic acute ischemic kidney injury.Front Cell Dev Biol. 2025 May 22;13:1494660. doi: 10.3389/fcell.2025.1494660. eCollection 2025. Front Cell Dev Biol. 2025. PMID: 40476004 Free PMC article.
-
A proposed framework for advancing acute kidney injury risk stratification and diagnosis in children: a report from the 26th Acute Disease Quality Initiative (ADQI) conference.Pediatr Nephrol. 2024 Mar;39(3):929-939. doi: 10.1007/s00467-023-06133-3. Epub 2023 Sep 5. Pediatr Nephrol. 2024. PMID: 37670082 Free PMC article.
References
-
- Priyanka P, Zarbock A, Izawa J, Gleason TG, Renfurm RW, Kellum JA. The impact of acute kidney injury by serum creatinine or urine output criteria on major adverse kidney events in cardiac surgery patients. J Thorac Cardiovasc Surg. 2021;162(143–151):e147. - PubMed
-
- Nadim MK, Forni LG, Bihorac A, Hobson C, Koyner JL, Shaw A, Arnaoutakis GJ, Ding X, Engelman DT, Gasparovic H, et al. Cardiac and vascular surgery-associated acute kidney injury: the 20th International Consensus Conference of the ADQI (acute disease quality initiative) Group. J Am Heart Assoc. 2018;7:e008834. doi: 10.1161/JAHA.118.008834. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
