

Clinical outcomes in central nervous system solitary-fibrous tumor/hemangiopericytoma: a STROBE-compliant single-center analysis
- PMID: 35538540
- PMCID: PMC9088104
- DOI: 10.1186/s12957-022-02619-w
Clinical outcomes in central nervous system solitary-fibrous tumor/hemangiopericytoma: a STROBE-compliant single-center analysis
Abstract
Background: Solitary fibrous tumor (SFT) and hemangiopericytoma (HPC) are rare mesenchymal tumors in the central nervous system with a high tendency to relapse, having a significant impact on quality of life (QoL). Due to the rarity of intracranial SFT/HPC, the prognostic factors and optimal treatment remain to be elucidated. Meanwhile, quality of life in patients with intracranial SFT/HPC is seldomly concerned. Thus, we aim to survey about the quality of life and underline some aspects demanding concern in intracranial SFT/HPC treatment through summarizing our case series in recent ten years.
Methods: Patients with intracranial SFT/HPC who underwent surgical resection from January 2009 to June 2019 were included in the study. Clinical features, such as age, gender, and resection extent, were collected. The EuroQol Five Dimensions Questionnaire (EQ-5D) was used to assess the patients' quality of life (QoL). Prognosis factors related to progression-free survival (PFS) and overall survival (OS) were also evaluated.
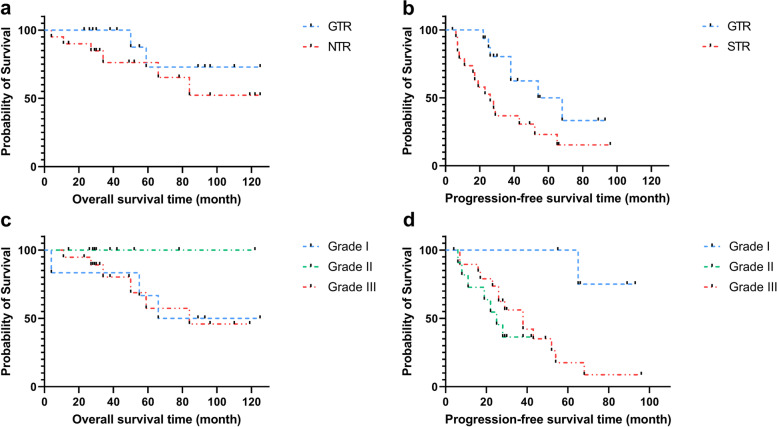
Results: Thirty-six patients with a mean follow-up period of 61.6 months (range 13-123 months) were included in this study. Sixteen (44.4%) patients achieved gross total resection (GTR). Fourteen patients (38.9%) with tumor progression experienced adjuvant radiotherapy (11.1%) or Gamma Knife surgery (GKS, 27.8%). According to the 2016 WHO classification, there were 6 (16.7%) grade I SFT/HPC, 11 (30.5%) grade II SFT/HPC, and 19 (52.8%) grade III SFT/HPC. The PFS and OS were 29 months (range 4-96 months) and 38 months (range 4-125 months). The median EQ5D-3 L tariff with or without progression was 0.617 (95% CI 0.470-0.756) and 0.939 (95% CI 0.772-0.977) respectively. Gross total resection (GTR, p = 0.024) and grade I SFT/HPC (p = 0.017) were significantly associated with longer PFS. In multivariate analysis, GTR (HR 0.378, 95% CI 0.154-0.927) and adjuvant therapy (HR 0.336, 95% CI 0.118-0.956) result in significantly longer PFS in patients with SFT/HPC.
Conclusions: Patients underwent GTR and adjuvant therapy had longer PFS. Similarly, patients with lower WHO grade had relatively longer PFS. Therefore, GTR is advocated for the treatment of SFT/HPC. And adjuvant therapy such as GKS could be an alternative treatment for patients who underwent STR or with tumor progression. Further, the QoL decreased in patients with tumor progression and metastasis, and more attention is demanded to the QoL of intracranial SFT/HPC patients.
Keywords: Central nervous system; Hemangiopericytoma; Prognosis; Quality of life; Solitary fibrous tumor.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Kim BS, Kim Y, Kong DS, Nam DH, Lee JI, Suh YL, Seol HJ. Clinical outcomes of intracranial solitary fibrous tumor and hemangiopericytoma: analysis according to the 2016 WHO classification of central nervous system tumors. J Neurosurg. 2018;129(6):1384–1396. doi: 10.3171/2017.7.JNS171226. - DOI - PubMed
-
- Zeng L, Wang Y, Wang Y, Han L, Niu H, Zhang M, Ke C, Chen J, Lei T. Analyses of prognosis-related factors of intracranial solitary fibrous tumors and hemangiopericytomas help understand the relationship between the two sorts of tumors. J Neurooncol. 2017;131(1):153–161. doi: 10.1007/s11060-016-2282-y. - DOI - PubMed
-
- Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta neuropathologica. 2016;131(6):803–820. doi: 10.1007/s00401-016-1545-1. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
