

Stent-assisted coiling of unruptured paraclinoid aneurysms with wide neck or unfavorable dome-to-neck ratio: Results of ventral wall vs dorsal wall with propensity score matching analysis
- PMID: 35538879
- PMCID: PMC11095348
- DOI: 10.1177/15910199221100966
Stent-assisted coiling of unruptured paraclinoid aneurysms with wide neck or unfavorable dome-to-neck ratio: Results of ventral wall vs dorsal wall with propensity score matching analysis
Abstract
Objective: This study aimed to evaluate the clinical safety and efficacy of stent-assisted coil embolization of unruptured wide-necked paraclinoid aneurysms based on the projection distribution.
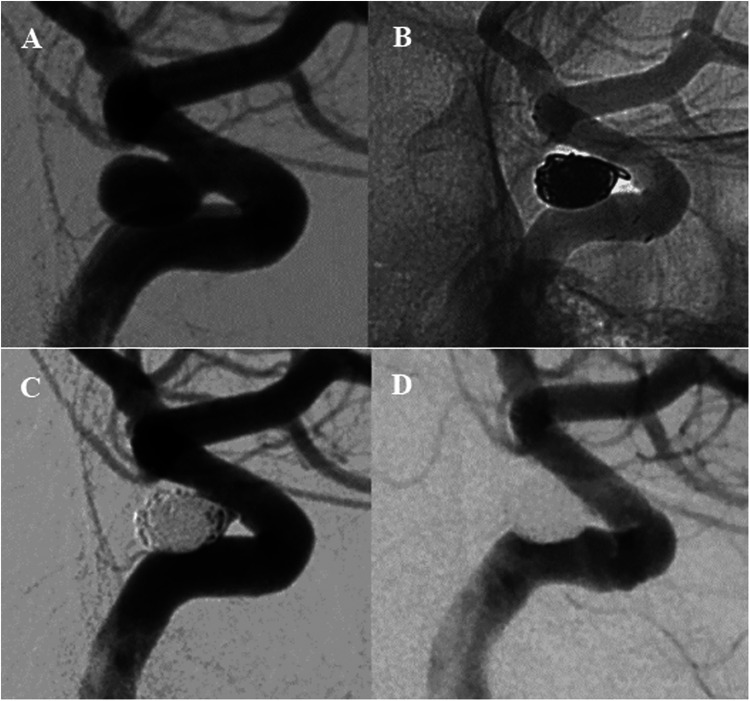
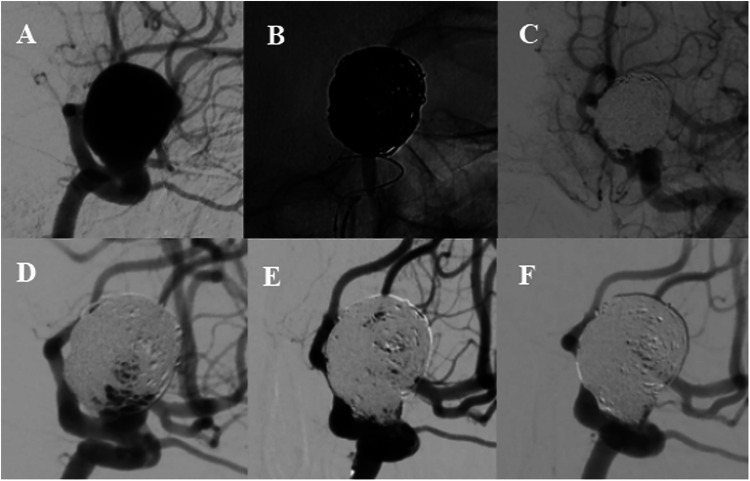
Methods: Between November 2015 and September 2020, 267 unruptured paraclinod aneurysms in 236 patients were identified with a wide neck or unfavorable dome-to-neck ratio and treated with stent-assisted coiling technique. The classification of this segment aneurysms was simplified to the dorsal group (located on the anterior wall) and ventral group (Non-dorsal). Following propensity score matching analysis, the clinical and radiographic data were compared between the two groups.
Results: Among 267 aneurysms, 186 were located on the ventral wall and 81 were on the dorsal wall. Dorsal wall aneurysms had a larger size (p < .001), wider neck (p = .001), and higher dome-to-neck ratio (p = .023) compared with ventral wall aneurysms. Propensity score-matched analysis found that dorsal group had a significantly higher likelihood of unfavorable results in immediate (residual sac, 39.4% vs. 18.2%, p = .007) and follow-up angiography (residual sac, 14.8% vs. 1.9%, p = .037) compared with ventral group, with significant difference in recurrence rates (9.3% vs. 0%, p = .028). The rates of procedure-related complications were not significantly different, but one thromboembolic event occurred in the dorsal group with clinical deterioration.
Conclusions: Traditional stent-assisted coiling can be given preference in paraclinoid aneurysms located on the ventral wall. The relatively high rate of recurrence in dorsal wall aneurysms with stent assistance may require other treatment options.
Keywords: Paraclinoid aneurysm; coil embolization; stent.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Day AL. Aneurysms of the ophthalmic segment. A clinical and anatomical analysis. J Neurosurg 1990; 72: 677–691. 1990/05/01. - PubMed
-
- Yadla S, Campbell PG, Grobelny B, et al. Open and endovascular treatment of unruptured carotid-ophthalmic aneurysms: clinical and radiographic outcomes. Neurosurgery 2011; 68: 1434–1443. discussion 1443. 2011/01/29. - PubMed
-
- De Jesus O, Sekhar LN, Riedel CJ. Clinoid and paraclinoid aneurysms: surgical anatomy, operative techniques, and outcome. Surg Neurol 1999; 51: 477–487. discussion 487–478. 1999/05/13. - PubMed
-
- Ogilvy CS, Natarajan SK, Jahshan S, et al. Stent-assisted coiling of paraclinoid aneurysms: risks and effectiveness. J Neurointerv Surg 2011; 3: 14–20. 2011/10/13. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
