

Single vs Dual-site service reconfiguration during Covid-19 pandemic - A tertiary care centre experience in hip fractures and a Scoping review
- PMID: 35540794
- PMCID: PMC9072772
- DOI: 10.1016/j.jcot.2022.101890
Single vs Dual-site service reconfiguration during Covid-19 pandemic - A tertiary care centre experience in hip fractures and a Scoping review
Abstract
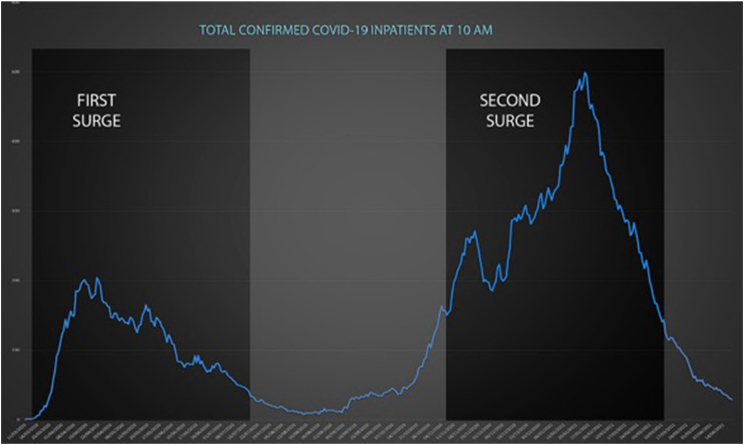
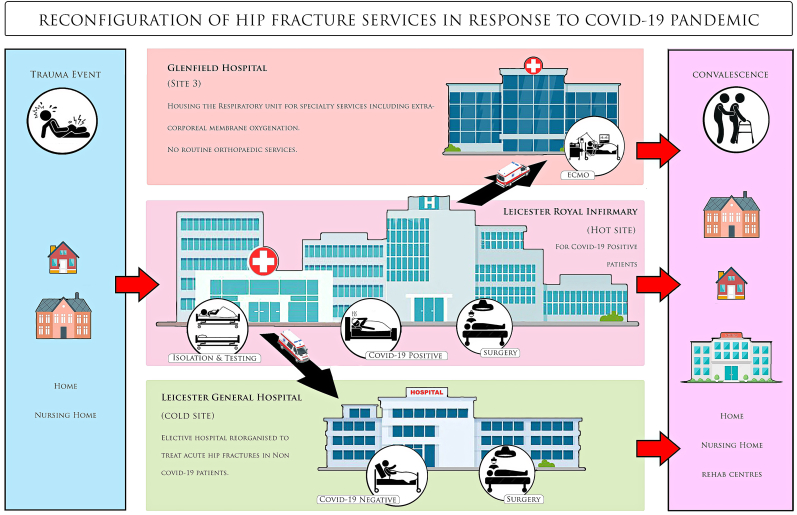
Aims and objectives: The Covid-19 pandemic has had an unprecedented effect on surgical practice and healthcare delivery globally. We compared the impact of the care pathways which segregate Covid-19 Positive and Negative patients into two geographically separate sites, on hip fracture patients in our high-volume trauma center in 3 distinct eras - the pre-pandemic period, against the first Covid-19 wave with dual-site service design, as well as the subsequent surge with single-site service delivery. In addition, we sought to invoke similar experiences of centres worldwide through a scoping literature review on the current evidence on "Dual site" reconfigurations in response to Covid-19 pandemic.
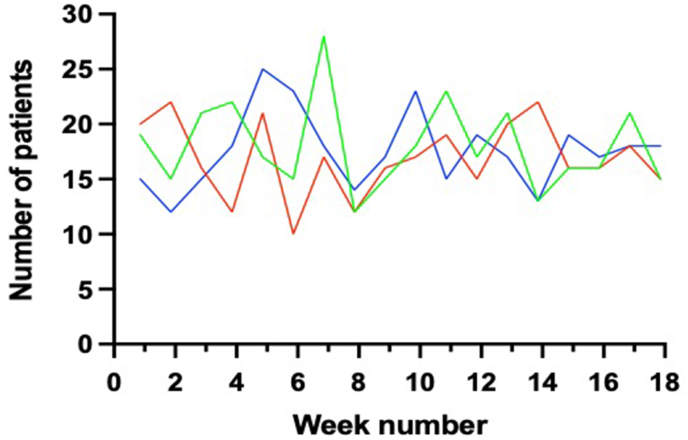
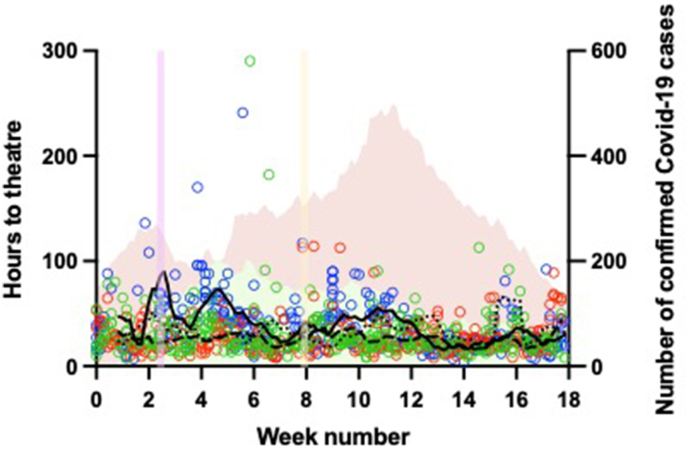
Methods: We prospectively reviewed our hip fracture patients throughout the two peaks of the pandemic, with different service designs for each, and compared the outcomes with a historic service provision. Further, a comprehensive literature search was conducted using several databases for articles discussing Dual-site service redesign.
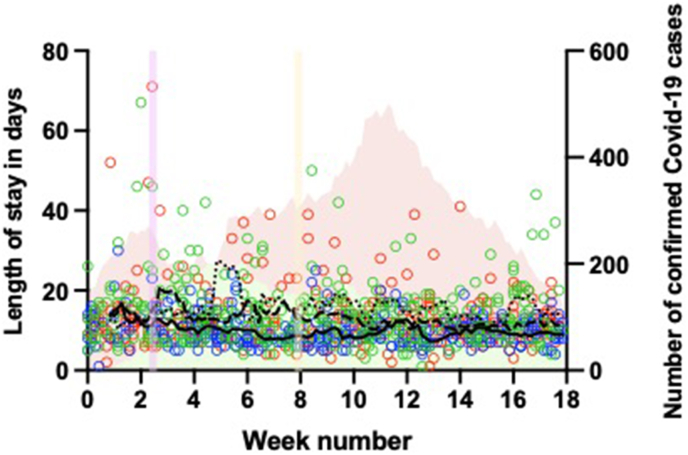
Results: In our in-house study, there was no statistically significant difference in mortality of hip fracture patients between the 3 periods, as well as their discharge destinations. With dual-site reconfiguration, patients took longer to reach theatre. However, there was much more nosocomial transmission with single-site service, and patients stayed in the hospital longer. 24 articles pertaining to the topic were selected for the scoping review. Most studies favour dual-site service reorganization, and reported beneficial outcomes from the detached care pathways.
Conclusion: It is safe to continue urgent as well as non-emergency surgery during the Covid-19 pandemic in a separate, geographically isolated site.
Crown Copyright © 2022 All rights reserved.
Conflict of interest statement
None of the authors have any conflicts of interest to declare. The study has been performed in accordance with the ethical standards of the institutional and Health Research Authority guidelines, as well as the Declaration of Helsinki and its further amendments.
Figures
References
-
- Natl. Hip Fract. Database. 2019. National hip fracture database annual report.
Publication types
LinkOut - more resources
Full Text Sources
