

Patterns of Skills Acquisition in Anesthesiologists During Simulated Interscalene Block Training on a Soft Embalmed Thiel Cadaver: Cohort Study
- PMID: 35543314
- PMCID: PMC9412904
- DOI: 10.2196/32840
Patterns of Skills Acquisition in Anesthesiologists During Simulated Interscalene Block Training on a Soft Embalmed Thiel Cadaver: Cohort Study
Abstract
Background: The demand for regional anesthesia for major surgery has increased considerably, but only a small number of anesthesiologists can provide such care. Simulations may improve clinical performance. However, opportunities to rehearse procedures are limited, and the clinical educational outcomes prescribed by the Royal College of Anesthesiologists training curriculum 2021 are difficult to attain. Educational paradigms, such as mastery learning and dedicated practice, are increasingly being used to teach technical skills to enhance skills acquisition. Moreover, high-fidelity, resilient cadaver simulators are now available: the soft embalmed Thiel cadaver shows physical characteristics and functional alignment similar to those of patients. Tissue elasticity allows tissues to expand and relax, fluid to drain away, and hundreds of repeated injections to be tolerated without causing damage. Learning curves and their intra- and interindividual dynamics have not hitherto been measured on the Thiel cadaver simulator using the mastery learning and dedicated practice educational paradigm coupled with validated, quantitative metrics, such as checklists, eye tracking metrics, and self-rating scores.
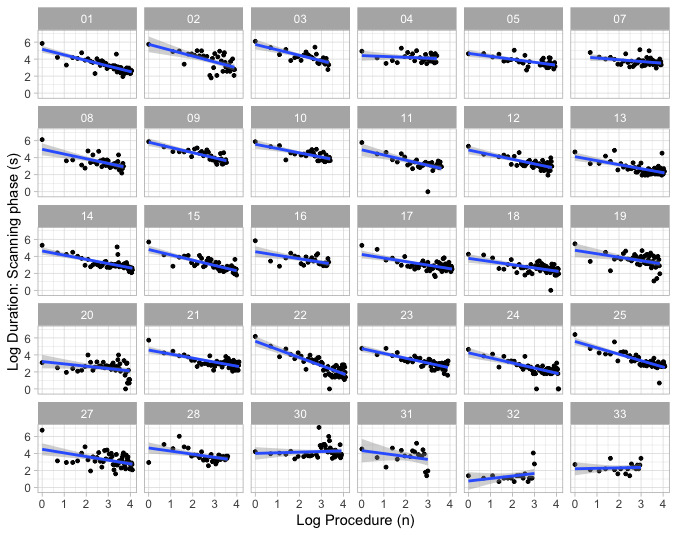
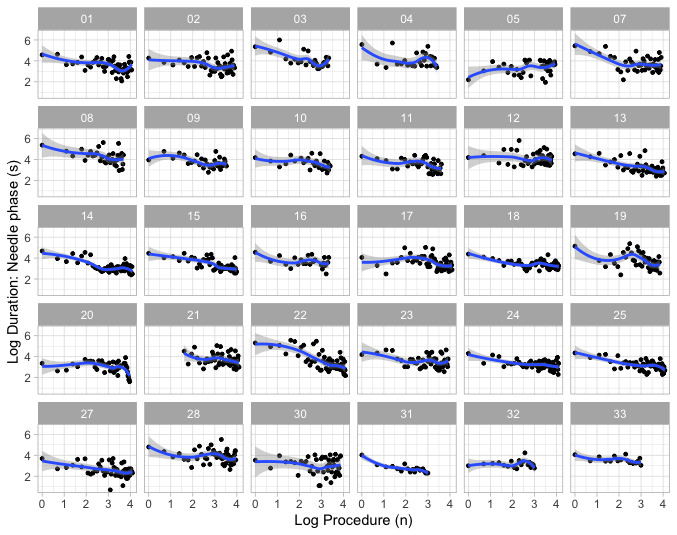
Objective: Our primary objective was to measure the learning slopes of the scanning and needling phases of an interscalene block conducted repeatedly on a soft embalmed Thiel cadaver over a 3-hour period of training.
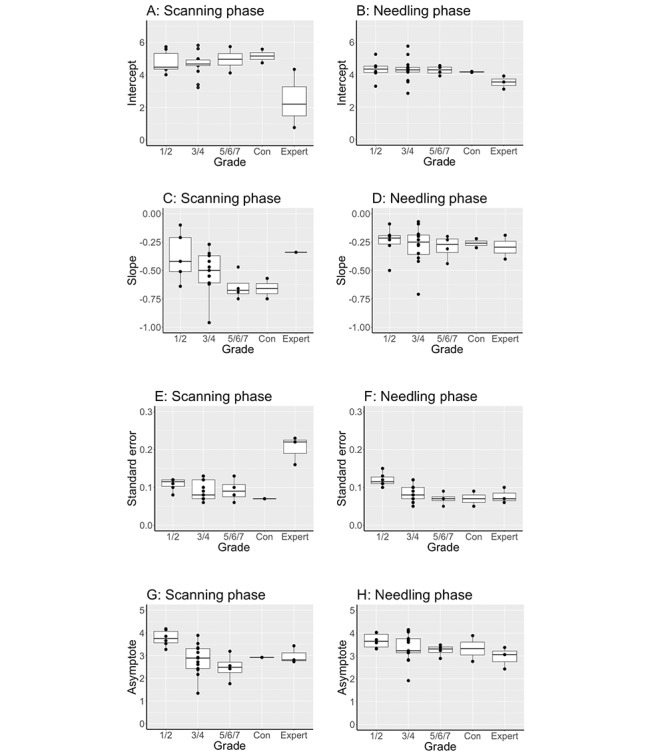
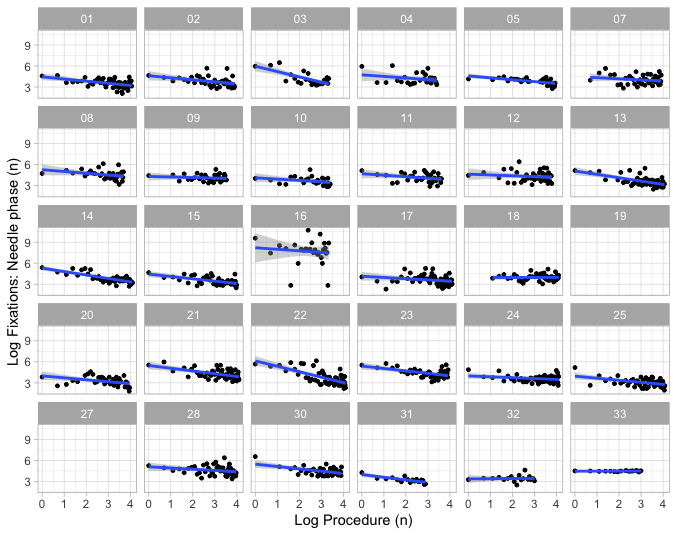
Methods: A total of 30 anesthesiologists, with a wide range of experience, conducted up to 60 ultrasound-guided interscalene blocks over 3 hours on the left side of 2 soft embalmed Thiel cadavers. The duration of the scanning and needling phases was defined as the time taken to perform all the steps correctly. The primary outcome was the best-fit linear slope of the log-log transformed time to complete each phase. Our secondary objectives were to measure preprocedural psychometrics, describe deviations from the learning slope, correlate scanning and needling phase data, characterize skills according to clinical grade, measure learning curves using objective eye gaze tracking and subjective self-rating measures, and use cluster analysis to categorize performance irrespective of grade.
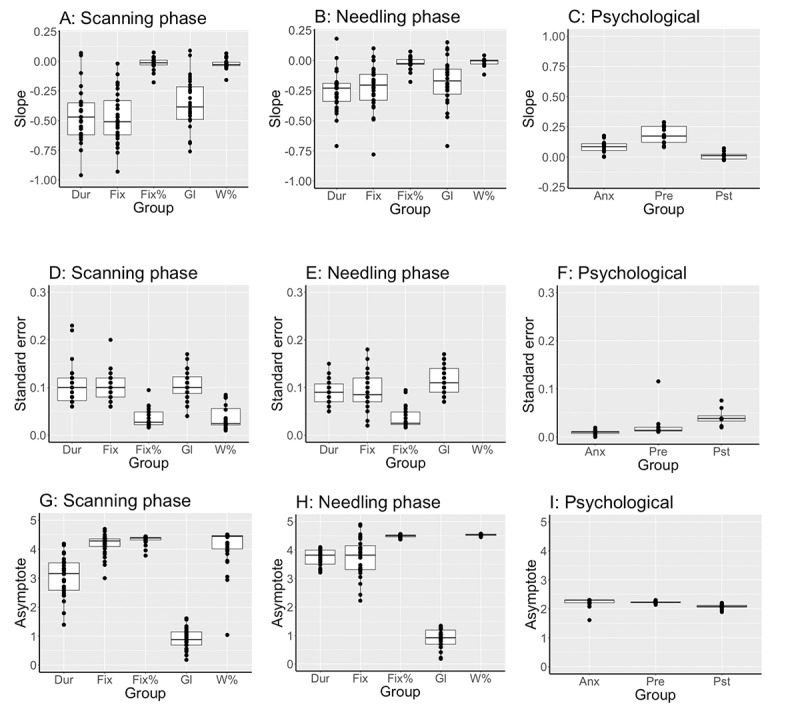
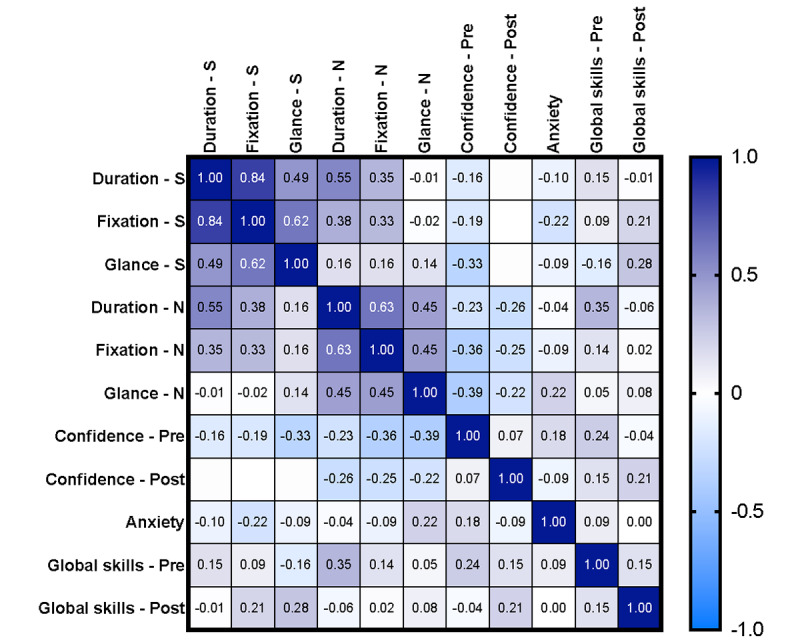
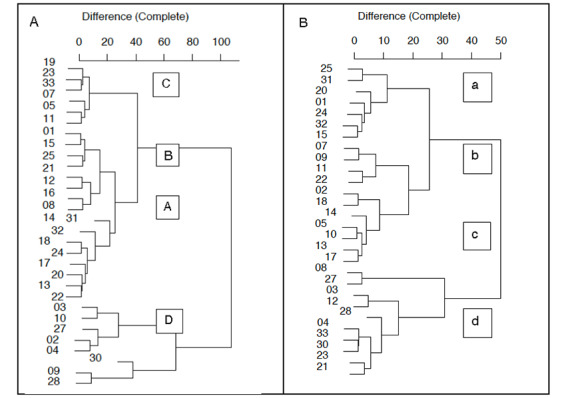
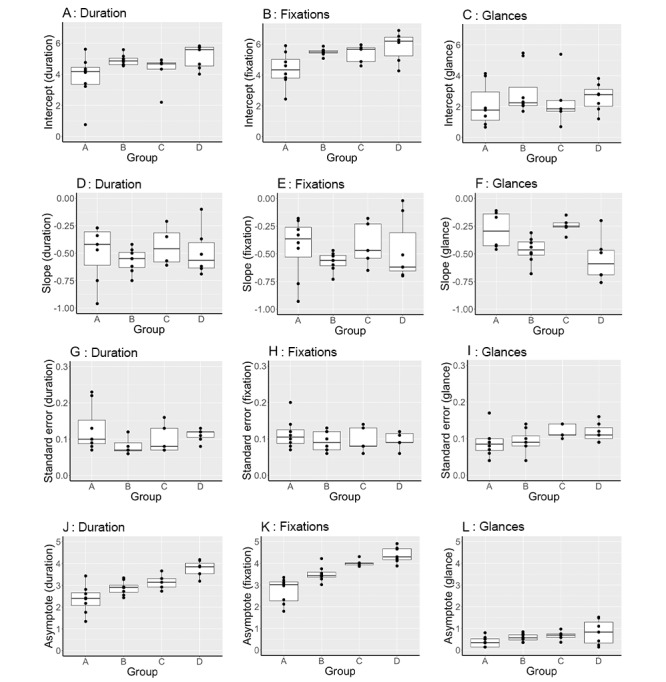
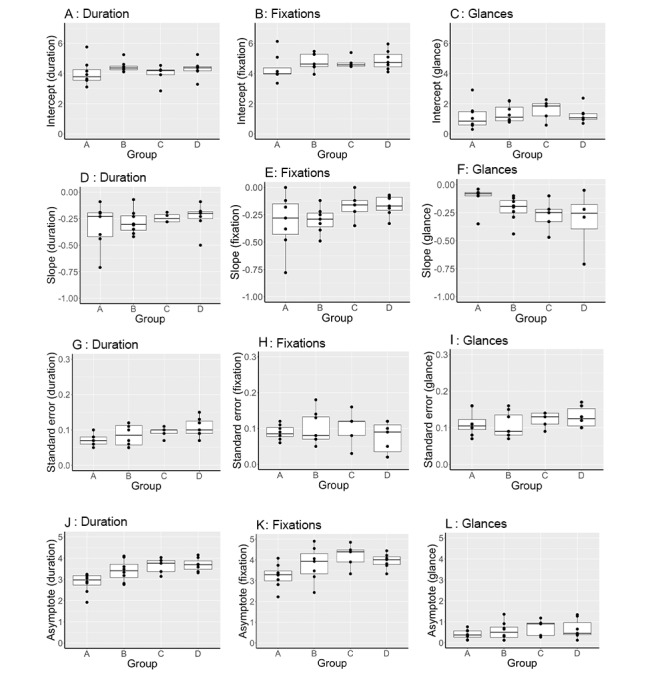
Results: The median (IQR; range) log-log learning slopes were -0.47 (-0.62 to -0.32; -0.96 to 0.30) and -0.23 (-0.34 to -0.19; -0.71 to 0.27) during the scanning and needling phases, respectively. Locally Weighted Scatterplot Smoother curves showed wide variability in within-participant performance. The learning slopes of the scanning and needling phases correlated: ρ=0.55 (0.23-0.76), P<.001, and ρ=-0.72 (-0.46 to -0.87), P<.001, respectively. Eye gaze fixation count and glance count during the scanning and needling phases best reflected block duration. Using clustering techniques, fixation count and glance were used to identify 4 distinct patterns of learning behavior.
Conclusions: We quantified learning slopes by log-log transformation of the time taken to complete the scanning and needling phases of interscalene blocks and identified intraindividual and interindividual patterns of variability.
Keywords: eye tracking; learning curves; regional anesthesia; simulation; ultrasonography.
©Graeme McLeod, Mel McKendrick, Tedis Tafili, Mateo Obregon, Ruth Neary, Ayman Mustafa, Pavan Raju, Donna Kean, Gary McKendrick, Tuesday McKendrick. Originally published in JMIR Medical Education (https://mededu.jmir.org), 11.08.2022.
Conflict of interest statement
Conflicts of Interest: MM is the chief executive officer of Optomize.
Figures
Similar articles
-
Physical properties and functional alignment of soft-embalmed Thiel human cadaver when used as a simulator for ultrasound-guided regional anaesthesia.Br J Anaesth. 2016 May;116(5):699-707. doi: 10.1093/bja/aev548. Br J Anaesth. 2016. PMID: 27106974
-
Validity and reliability of metrics for translation of regional anaesthesia performance from cadavers to patients.Br J Anaesth. 2019 Sep;123(3):368-377. doi: 10.1016/j.bja.2019.04.060. Epub 2019 Jun 27. Br J Anaesth. 2019. PMID: 31255289
-
Validation of the soft-embalmed Thiel cadaver as a high-fidelity simulator of pressure during targeted nerve injection.Reg Anesth Pain Med. 2021 Jun;46(6):540-548. doi: 10.1136/rapm-2020-102132. Epub 2021 Apr 27. Reg Anesth Pain Med. 2021. PMID: 33906953
-
Quantitative assessment of Thiel soft-embalmed human cadavers using shear wave elastography.Ann Anat. 2015 Nov;202:52-6. doi: 10.1016/j.aanat.2015.06.007. Epub 2015 Aug 24. Ann Anat. 2015. PMID: 26342463
-
Benefits and Pitfalls of Cadavers as Learning Tool for Ultrasound-guided Regional Anesthesia.Anesth Essays Res. 2017 Jan-Mar;11(1):3-6. doi: 10.4103/0259-1162.186607. Anesth Essays Res. 2017. PMID: 28298747 Free PMC article. Review.
Cited by
-
Development and validation of metrics for assessment of ultrasound-guided fascial block skills☆.Br J Anaesth. 2024 Oct;133(4):862-873. doi: 10.1016/j.bja.2024.06.039. Epub 2024 Aug 8. Br J Anaesth. 2024. PMID: 39117476
-
Research priorities in regional anaesthesia: an international Delphi study.Br J Anaesth. 2024 May;132(5):1041-1048. doi: 10.1016/j.bja.2024.01.033. Epub 2024 Mar 5. Br J Anaesth. 2024. PMID: 38448274 Free PMC article. Review.
-
Hologram-assisted thoracic epidural insertion in the Thiel soft embalmed cadaver: proof of concept simulation study.Br J Anaesth. 2025 Mar;134(3):865-867. doi: 10.1016/j.bja.2024.11.039. Epub 2025 Jan 22. Br J Anaesth. 2025. PMID: 39848873 Free PMC article. No abstract available.
-
Improved Post-Operative Outcomes and Reduced Narcotic Use With ERAS Protocol in a Pediatric Ambulatory Surgery Setting.Paediatr Neonatal Pain. 2025 Mar 10;7(1):e70004. doi: 10.1002/pne2.70004. eCollection 2025 Mar. Paediatr Neonatal Pain. 2025. PMID: 40066436 Free PMC article.
References
-
- Neal JM, Brull R, Horn JL, Liu SS, McCartney CJ, Perlas A, Salinas FV, Tsui BC. The second American society of regional anesthesia and pain medicine evidence-based medicine assessment of ultrasound-guided regional anesthesia: executive summary. Reg Anesth Pain Med. 2016;41(2):181–94. doi: 10.1097/AAP.0000000000000331. - DOI - PubMed
-
- Uppal V, Sondekoppam RV, Landau R, El-Boghdadly K, Narouze S, Kalagara HK. Neuraxial anaesthesia and peripheral nerve blocks during the COVID-19 pandemic: a literature review and practice recommendations. Anaesthesia. 2020 Oct;75(10):1350–63. doi: 10.1111/anae.15105. doi: 10.1111/anae.15105. - DOI - DOI - PMC - PubMed
-
- Borg LK, Harrison TK, Kou A, Mariano ER, Udani AD, Kim TE, Shum C, Howard SK, ADAPT (Anesthesiology-Directed Advanced Procedural Training) Research Group Preliminary experience using eye-tracking technology to differentiate novice and expert image interpretation for ultrasound-guided regional anesthesia. J Ultrasound Med. 2018 Feb;37(2):329–36. doi: 10.1002/jum.14334. - DOI - PubMed
-
- McKendrick M, Sadler A, Taylor A, Seeley J, Filipescu T, Mustafa A, McKendrick G, Halcrow J, Raju P, McLeod GA. The effect of an ultrasound-activated needle tip tracker needle on the performance of sciatic nerve block on a soft embalmed Thiel cadaver. Anaesthesia. 2021 Feb;76(2):209–17. doi: 10.1111/anae.15211. doi: 10.1111/anae.15211. - DOI - DOI - PubMed
LinkOut - more resources
Full Text Sources
