

Imaging incidental adrenal lesions
- PMID: 35543634
- PMCID: PMC9975514
- DOI: 10.1259/bjr.20220281
Imaging incidental adrenal lesions
Abstract
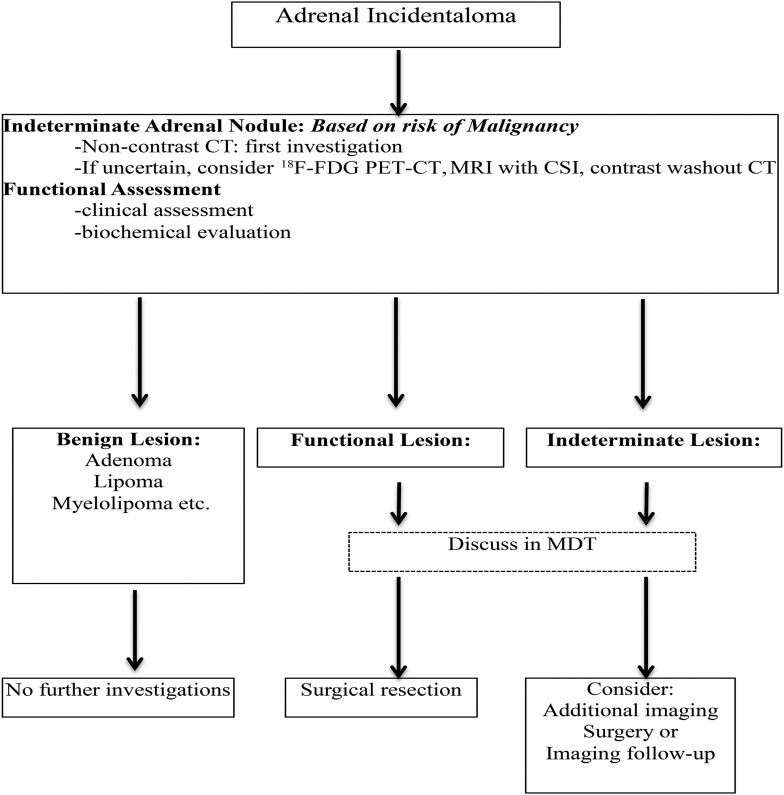
Incidental adrenal masses are among the most common incidental lesions detected on cross-sectional imaging. The majority are benign lesions, adenomas and myelolipomas being the most common. Simple cross-sectional imaging techniques using CT and MRI permit the characterization of over 80%, thereby requiring no further imaging. The remaining lesions are considered indeterminate. These lesions consist of benign and malignant lesions sharing imaging features. Further imaging and management of these indeterminate lesions should be guided by close collaboration between different specialists in an MDT setting. Advanced imaging options include dedicated adrenal scintigraphy, positron emission tomography CT, biopsy and surveillance. Biochemical and hormonal evaluation is also important to identify hyperfunctioning adrenal lesions. This review focuses on imaging features of benign and malignant adrenal masses used for characterization and suggests an imaging pathway for indeterminate adrenal masses.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
