

Frequency of transmission, asymptomatic shedding, and airborne spread of Streptococcus pyogenes in schoolchildren exposed to scarlet fever: a prospective, longitudinal, multicohort, molecular epidemiological, contact-tracing study in England, UK
- PMID: 35544097
- PMCID: PMC9042792
- DOI: 10.1016/S2666-5247(21)00332-3
Frequency of transmission, asymptomatic shedding, and airborne spread of Streptococcus pyogenes in schoolchildren exposed to scarlet fever: a prospective, longitudinal, multicohort, molecular epidemiological, contact-tracing study in England, UK
Abstract
Background: Despite recommendations regarding prompt treatment of cases and enhanced hygiene measures, scarlet fever outbreaks increased in England between 2014 and 2018. We aimed to assess the effects of standard interventions on transmission of Streptococcus pyogenes to classroom contacts, households, and classroom environments to inform future guidance.
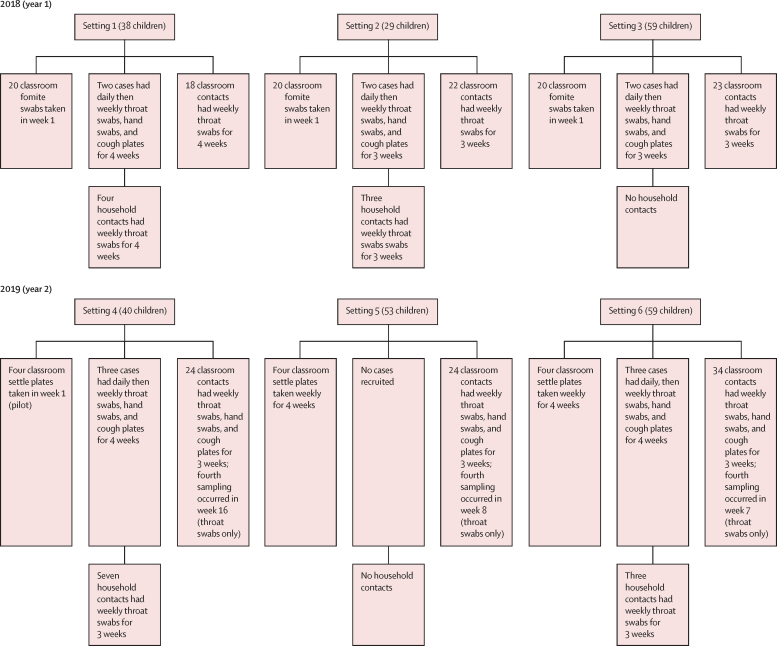
Methods: We did a prospective, longitudinal, multicohort, molecular epidemiological, contact-tracing study in six settings across five schools in Greater London, UK. Schools and nurseries were eligible to participate if they had reported two cases of scarlet fever within 10 days of each other among children aged 2-8 years from the same class, with the most recent case arising in the preceding 48 h. We cultured throat swabs from children with scarlet fever, classroom contacts, and household contacts at four timepoints. We also cultured hand swabs and cough plates from all cases in years 1 and 2 of the study, and from classroom contacts in year 2. Surface swabs from toys and other fomites in classrooms were cultured in year 1, and settle plates from classrooms were collected in year 2. Any sample with S pyogenes detected was recorded as positive and underwent emm genotyping and genome sequencing to compare with the outbreak strain.
Findings: Six classes, comprising 12 cases of scarlet fever, 17 household contacts, and 278 classroom contacts were recruited between March 1 and May 31, 2018 (year 1), and between March 1 and May 31, 2019 (year 2). Asymptomatic throat carriage of the outbreak strains increased from 11 (10%) of 115 swabbed children in week 1, to 34 (27%) of 126 in week 2, to 26 (24%) of 108 in week 3, and then five (14%) of 35 in week 4. Compared with carriage of outbreak S pyogenes strains, colonisation with non-outbreak and non-genotyped S pyogenes strains occurred in two (2%) of 115 swabbed children in week 1, five (4%) of 126 in week 2, six (6%) of 108 in week 3, and in none of the 35 children in week 4 (median carriage for entire study 2·8% [IQR 0·0-6·6]). Genome sequencing showed clonality of outbreak isolates within each of six classes, confirming that recent transmission accounted for high carriage. When transmissibility was tested, one (9%) of 11 asymptomatic carriers of emm4 and five (36%) of 14 asymptomatic carriers of emm3.93 had a positive cough plate. The outbreak strain was identified in only one (2%) of 60 surface swabs taken from three classrooms; however, in the two classrooms with settle plates placed in elevated locations, two (17%) of 12 and six (50%) of 12 settle plates yielded the outbreak strain.
Interpretation: Transmission of S pyogenes in schools is intense and might occur before or despite reported treatment of cases, underlining a need for rapid case management. Despite guideline adherence, heavy shedding of S pyogenes by few classroom contacts might perpetuate outbreaks, and airborne transmission has a plausible role in its spread. These findings highlight the need for research to improve understanding and to assess effectiveness of interventions to reduce airborne transmission of S pyogenes.
Funding: Action Medical Research, UK Research Innovation, and National Institute for Health Research.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures


Comment in
-
Strep A treatment, working for now.Lancet Microbe. 2023 Jan;4(1):e1. doi: 10.1016/S2666-5247(22)00360-3. Epub 2022 Dec 21. Lancet Microbe. 2023. PMID: 36565711 No abstract available.
References
-
- Guy R, Williams C, Irvine N, et al. Increase in scarlet fever notifications in the United Kingdom, 2013/2014. Euro Surveill. 2014;19 - PubMed
-
- Lamagni T, Guy R, Chand M, et al. Resurgence of scarlet fever in England, 2014-16: a population-based surveillance study. Lancet Infect Dis. 2018;18:180–187. - PubMed
-
- Public Health England Group A streptococcal infections: first report of seasonal activity, 2018/19. https://assets.publishing.service.gov.uk/government/uploads/system/uploa...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
