

Neuropsychiatric Ramifications of Severe COVID-19 and Other Severe Acute Respiratory Infections
- PMID: 35544272
- PMCID: PMC9096686
- DOI: 10.1001/jamapsychiatry.2022.1067
Neuropsychiatric Ramifications of Severe COVID-19 and Other Severe Acute Respiratory Infections
Abstract
Importance: Individuals surviving severe COVID-19 may be at increased risk of neuropsychiatric sequelae. Robust assessment of these risks may help improve clinical understanding of the post-COVID syndrome, aid clinical care during the ongoing pandemic, and inform postpandemic planning.
Objective: To quantify the risks of new-onset neuropsychiatric conditions and new neuropsychiatric medication prescriptions after discharge from a COVID-19-related hospitalization, and to compare these with risks after discharge from hospitalization for other severe acute respiratory infections (SARI) during the COVID-19 pandemic.
Design, setting, and participants: In this cohort study, adults (≥18 years of age) were identified from QResearch primary care and linked electronic health record databases, including national SARS-CoV-2 testing, hospital episode statistics, intensive care admissions data, and mortality registers in England, from January 24, 2020, to July 7, 2021.
Exposures: COVID-19-related or SARI-related hospital admission (including intensive care admission).
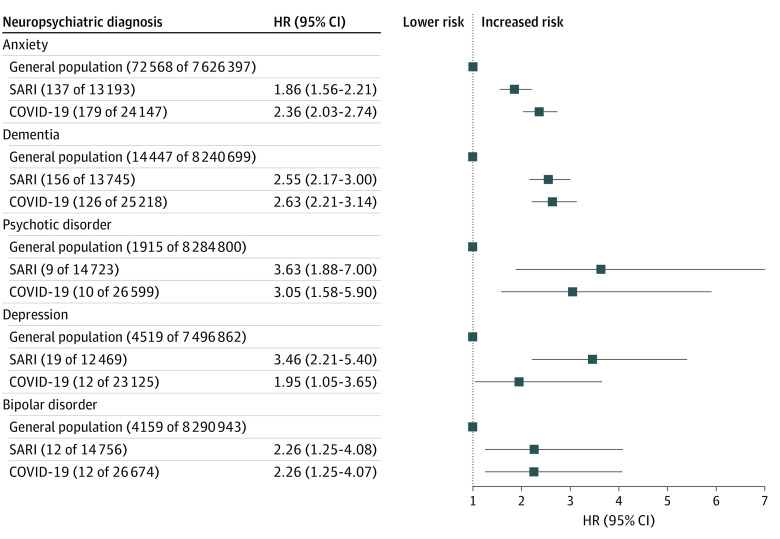
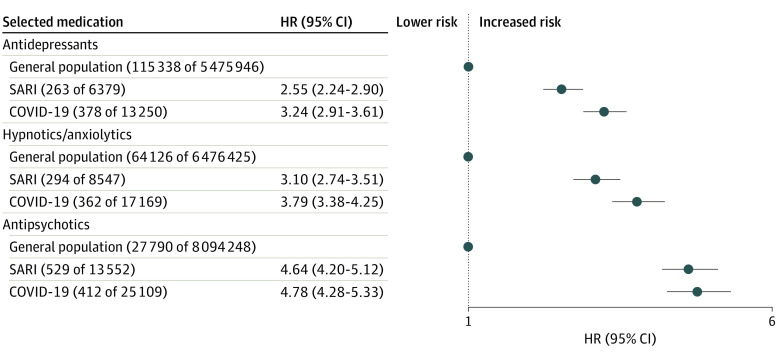
Main outcomes and measures: New-onset diagnoses of neuropsychiatric conditions (anxiety, dementia, psychosis, depression, bipolar disorder) or first prescription for relevant medications (antidepressants, hypnotics/anxiolytics, antipsychotics) during 12 months of follow-up from hospital discharge. Maximally adjusted hazard ratios (HR) with 95% CIs were estimated using flexible parametric survival models.
Results: In this cohort study of data from 8.38 million adults (4.18 million women, 4.20 million men; mean [SD] age 49.18 [18.45] years); 16 679 (0.02%) survived a hospital admission for SARI, and 32 525 (0.03%) survived a hospital admission for COVID-19. Compared with the remaining population, survivors of SARI and COVID-19 hospitalization had higher risks of subsequent neuropsychiatric diagnoses. For example, the HR for anxiety in survivors of SARI was 1.86 (95% CI, 1.56-2.21) and for survivors of COVID-19 infection was 2.36 (95% CI, 2.03-2.74); the HR for dementia for survivors of SARI was 2.55 (95% CI, 2.17-3.00) and for survivors of COVID-19 infection was 2.63 (95% CI, 2.21-3.14). Similar findings were observed for all medications analyzed; for example, the HR for first prescriptions of antidepressants in survivors of SARI was 2.55 (95% CI, 2.24-2.90) and for survivors of COVID-19 infection was 3.24 (95% CI, 2.91-3.61). There were no significant differences observed when directly comparing the COVID-19 group with the SARI group apart from a lower risk of antipsychotic prescriptions in the former (HR, 0.80; 95% CI, 0.69-0.92).
Conclusions and relevance: In this cohort study, the neuropsychiatric sequelae of severe COVID-19 infection were found to be similar to those for other SARI. This finding may inform postdischarge support for people surviving SARI.
Conflict of interest statement
Figures
References
-
- Johns Hopkins Coronavirus Resource Center . COVID-19 map. Accessed March 1, 2022. https://coronavirus.jhu.edu/map.html.
-
- Pandharipande PP, Girard TD, Ely EW. Long-term cognitive impairment after critical illness. N Engl J Med. 2014;370(2):185-186. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
