

Urea levels and cardiovascular disease in patients with chronic kidney disease
- PMID: 35544273
- PMCID: PMC9869852
- DOI: 10.1093/ndt/gfac045
Urea levels and cardiovascular disease in patients with chronic kidney disease
Abstract
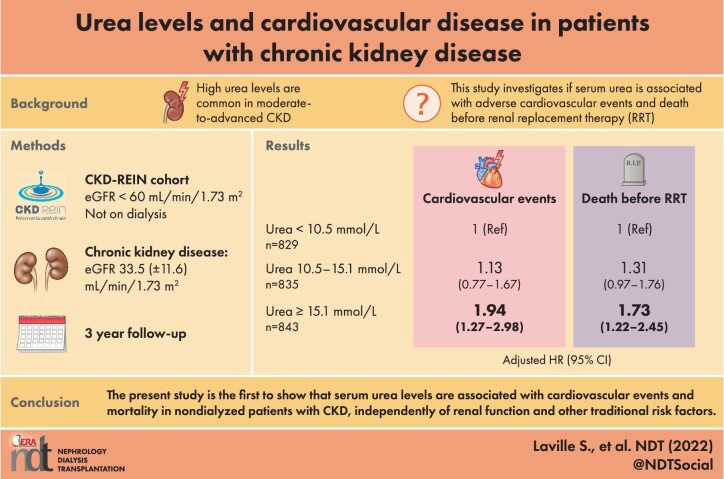
Background: Elevated serum urea levels are common in moderate-to-advanced CKD. Several studies have shown that urea is a direct and indirect uremic toxin, especially with regard to cardiovascular disease. We sought to determine whether serum urea levels are associated with adverse cardiovascular events and death before renal replacement therapy (RRT) in patients with CKD.
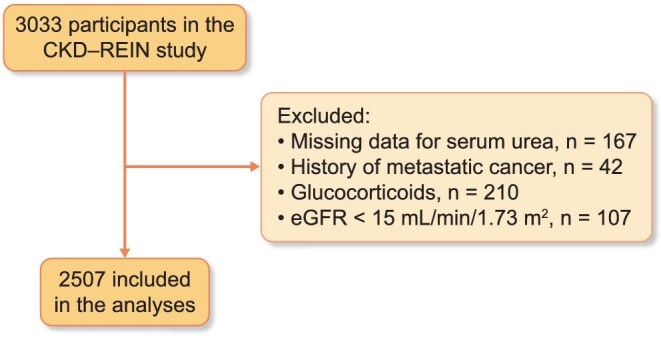
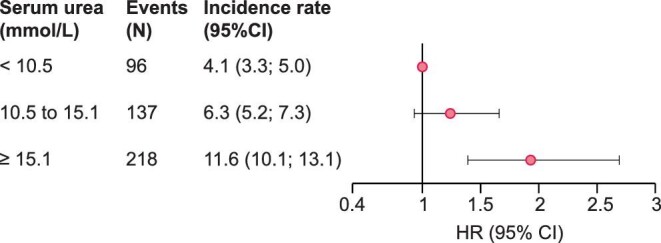
Methods: CKD-REIN is a prospective cohort of CKD nephrology outpatients not receiving maintenance dialysis. The 2507 patients included in the analysis were divided into three groups according to the baseline serum urea level (T1 < 10.5, T2:10.5 to 15.1, and T3 ≥ 15.1 mmol/L). Cox proportional hazard models were used to estimate hazard ratios (HRs) for first atheromatous or nonatheromatous cardiovascular (CV) events, and all-cause mortality before RRT. The models were adjusted for baseline comorbidities, laboratory data, and medications.
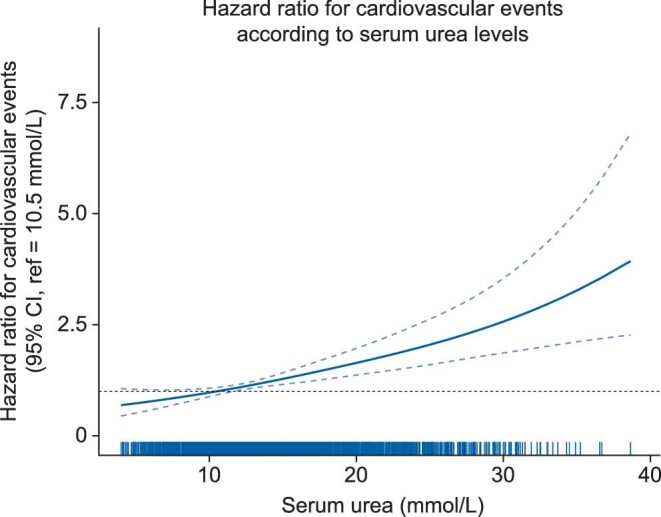
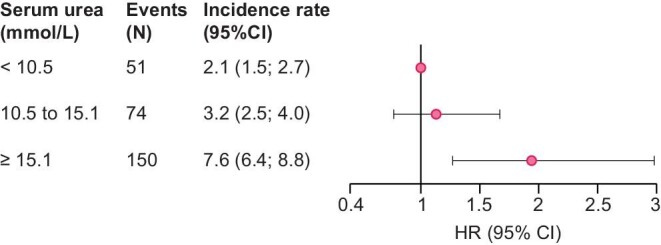
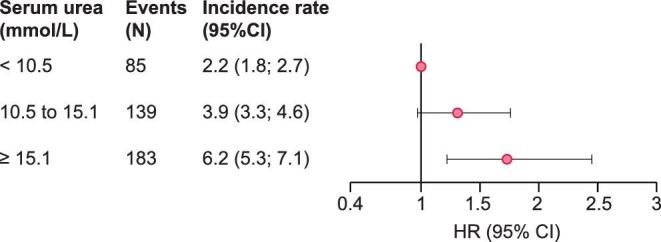
Findings: Of the 2507 included patients (median [interquartile range (IQR)] age: 69[61-77]; mean (standard deviation) eGFR 33.5(11.6) mL/min/1.73 m²), 54% had a history of cardiovascular disease. After multiple adjustments for cardiovascular risk factors (including eGFR), patients in T3 had a higher risk of atheromatous and nonatheromatous cardiovascular events than patient in T1 (n events = 451, HR[95%CI]: 1.93[1.39-2.69]). The adjusted HRs for death before RRT (n events = 407) were 1.31[0.97; 1.76] and 1.73[1.22; 2.45] for patients T2 and those in T3, respectively.
Interpretation: Our data suggested that urea is a predictor of cardiovascular outcomes beyond CV risk factors including eGFR.
Keywords: cardiovascular disease; chronic kidney disease; urea; uremic toxin.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Figures
References
-
- Levey AS, Atkins R, Coresh Jet al. Chronic kidney disease as a global public health problem: approaches and initiatives – a position statement from kidney disease improving global outcomes. Kidney Int 2007; 72: 247–259 - PubMed
-
- Jha V, Garcia-Garcia G, Iseki Ket al. Chronic kidney disease: global dimension and perspectives. Lancet North Am Ed 2013; 382: 260–272 - PubMed
-
- Go AS, Chertow GM, Fan Det al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 2004; 351: 1296–1305 - PubMed
-
- Vanholder R, Massy Z, Argiles Aet al. Chronic kidney disease as cause of cardiovascular morbidity and mortality. Nephrol Dial Transplant 2005; 20: 1048–1056 - PubMed
-
- Massy ZA, Pietrement C, Touré F. Reconsidering the lack of urea toxicity in dialysis patients. Semin Dial 2016; 29: 333–337 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
