

Acute inflammatory response via neutrophil activation protects against the development of chronic pain
- PMID: 35544595
- PMCID: PMC10317000
- DOI: 10.1126/scitranslmed.abj9954
Acute inflammatory response via neutrophil activation protects against the development of chronic pain
Abstract
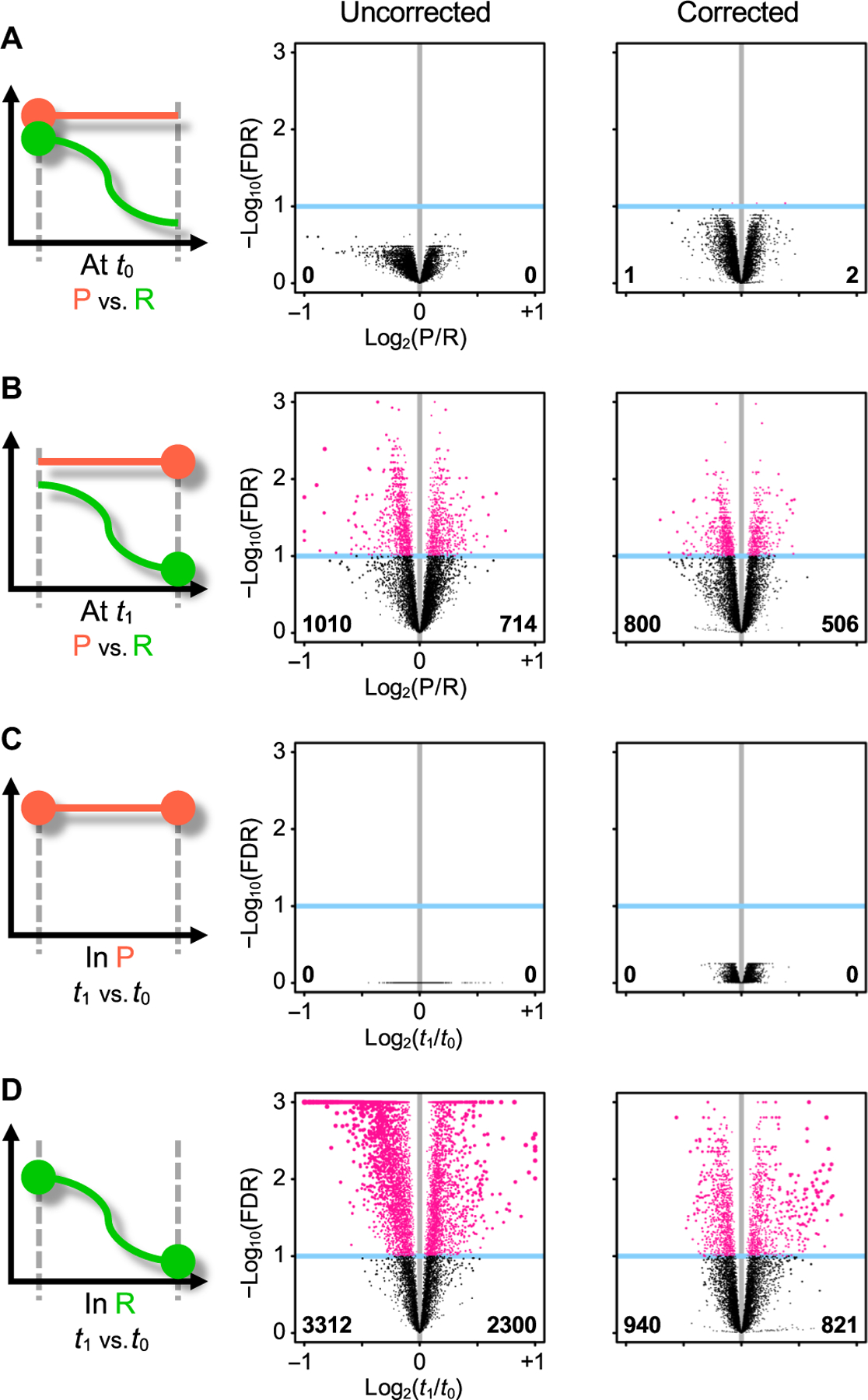
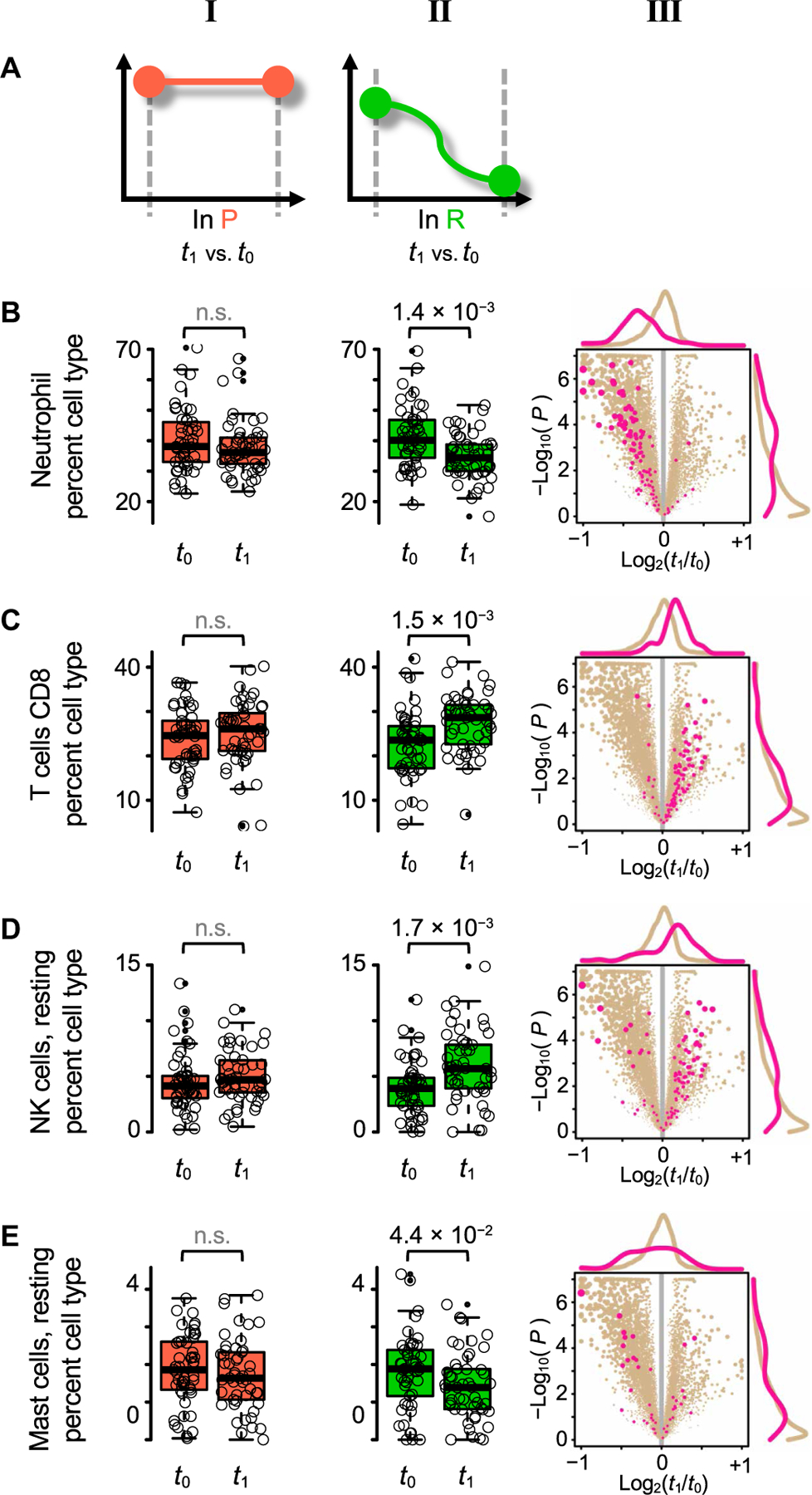
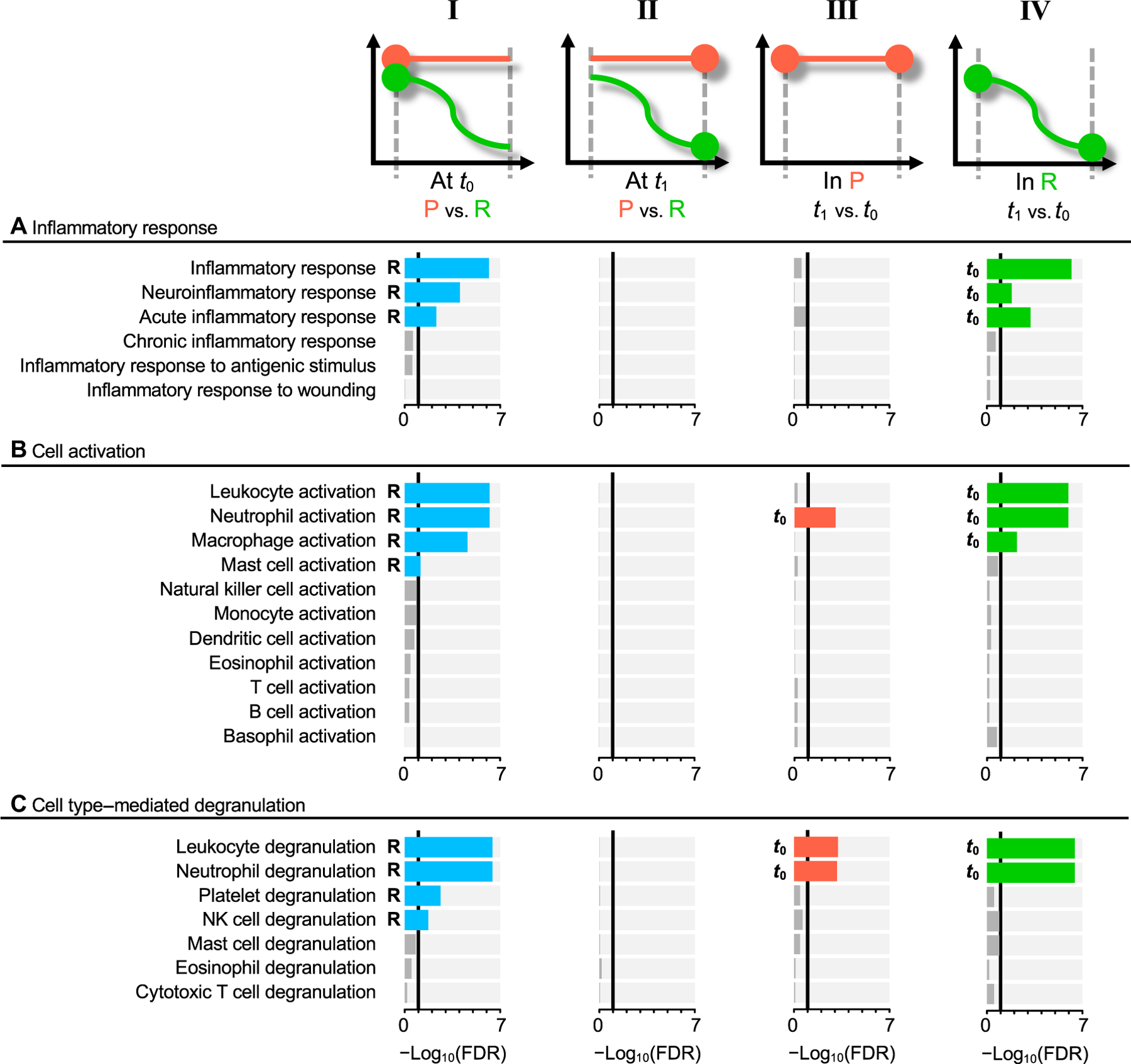
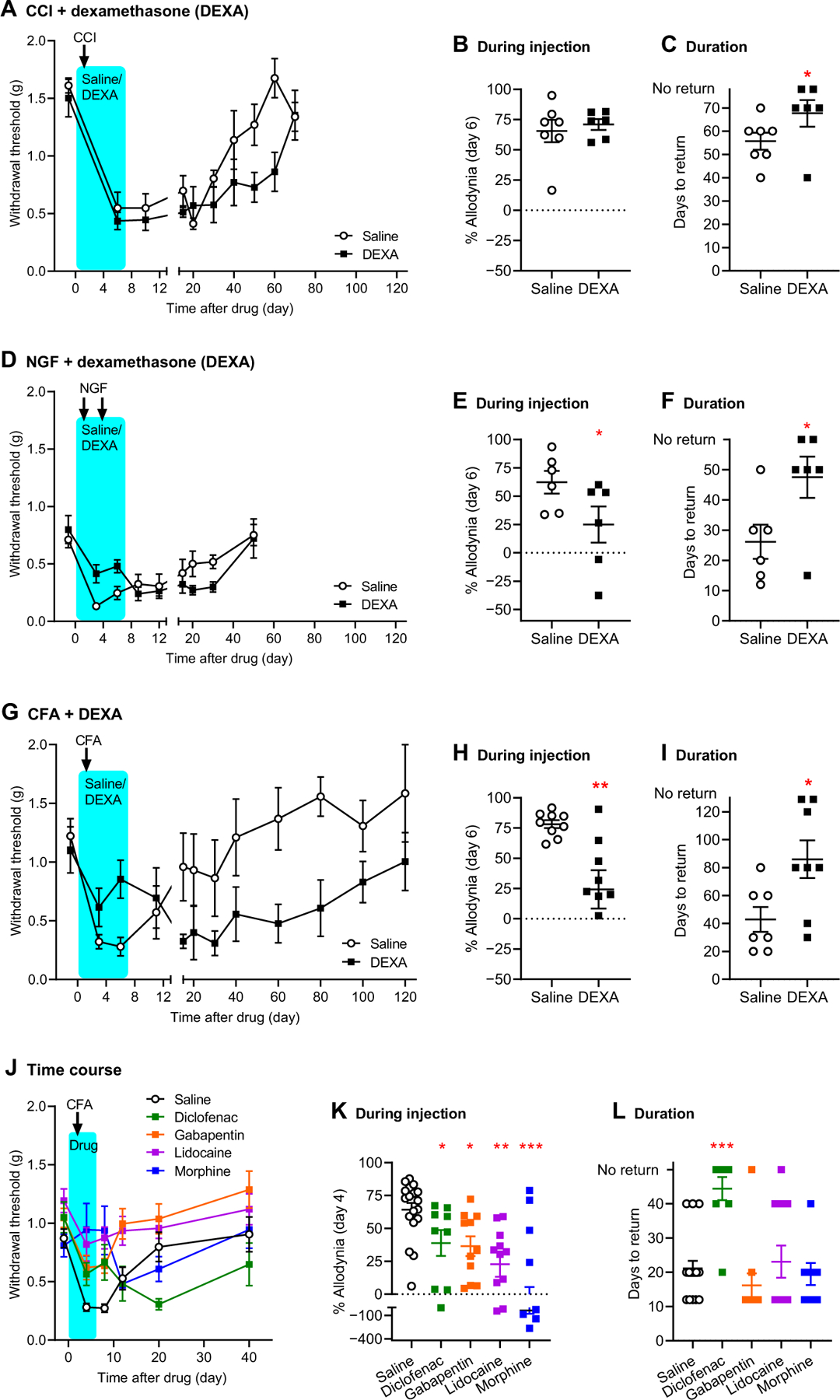
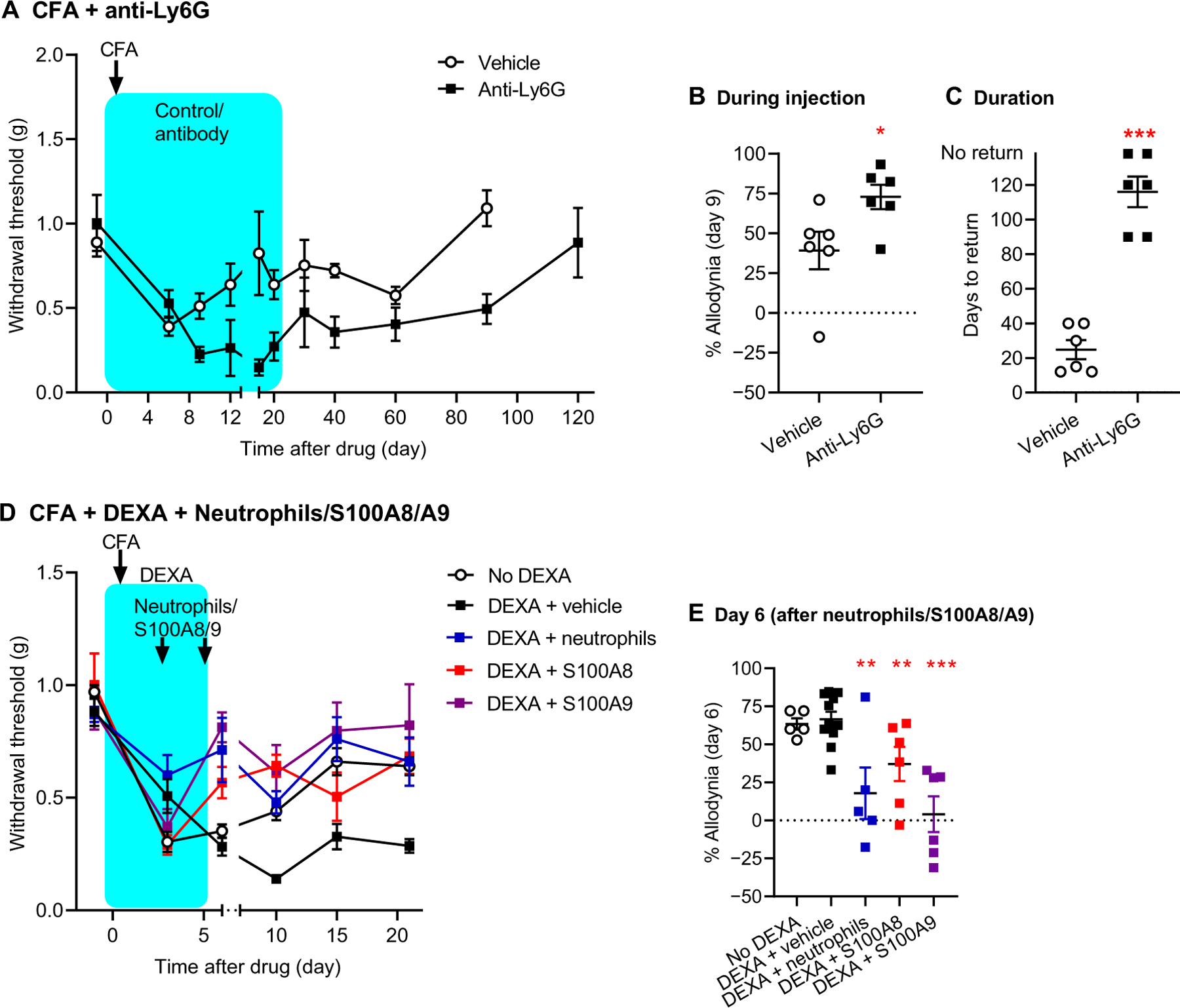
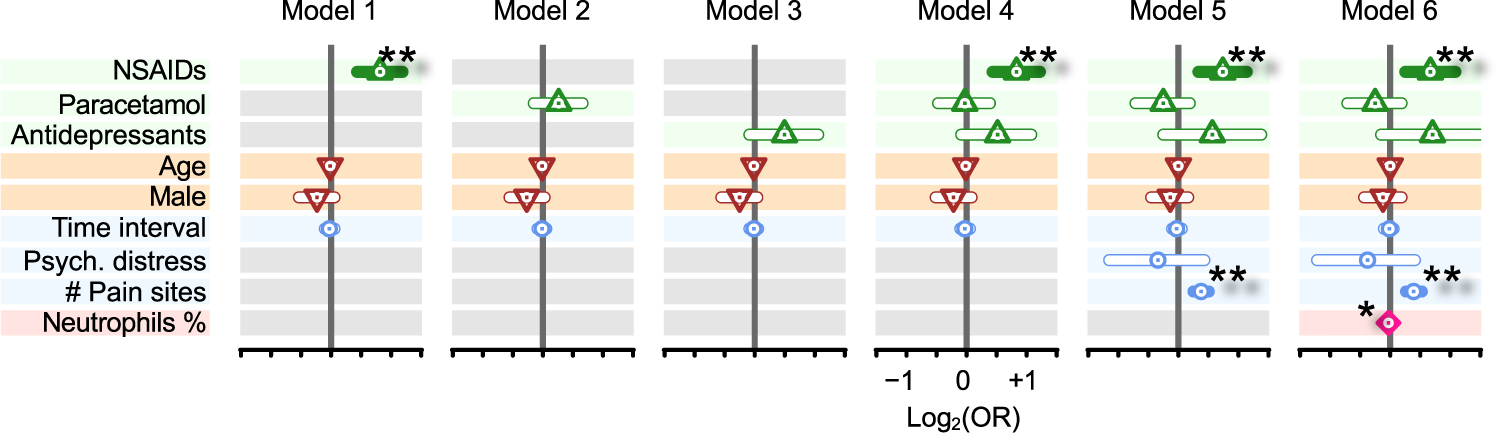
The transition from acute to chronic pain is critically important but not well understood. Here, we investigated the pathophysiological mechanisms underlying the transition from acute to chronic low back pain (LBP) and performed transcriptome-wide analysis in peripheral immune cells of 98 participants with acute LBP, followed for 3 months. Transcriptomic changes were compared between patients whose LBP was resolved at 3 months with those whose LBP persisted. We found thousands of dynamic transcriptional changes over 3 months in LBP participants with resolved pain but none in those with persistent pain. Transient neutrophil-driven up-regulation of inflammatory responses was protective against the transition to chronic pain. In mouse pain assays, early treatment with a steroid or nonsteroidal anti-inflammatory drug (NSAID) also led to prolonged pain despite being analgesic in the short term; such a prolongation was not observed with other analgesics. Depletion of neutrophils delayed resolution of pain in mice, whereas peripheral injection of neutrophils themselves, or S100A8/A9 proteins normally released by neutrophils, prevented the development of long-lasting pain induced by an anti-inflammatory drug. Analysis of pain trajectories of human subjects reporting acute back pain in the UK Biobank identified elevated risk of pain persistence for subjects taking NSAIDs. Thus, despite analgesic efficacy at early time points, the management of acute inflammation may be counterproductive for long-term outcomes of LBP sufferers.
Conflict of interest statement
Figures
Comment in
-
Anti-inflammatory drugs could cause chronic pain.Nat Rev Neurol. 2022 Jul;18(7):382. doi: 10.1038/s41582-022-00676-z. Nat Rev Neurol. 2022. PMID: 35610352 No abstract available.
-
[No evidence for advising against use of anti-inflammatory medications].Tidsskr Nor Laegeforen. 2022 Oct 24;142(15). doi: 10.4045/tidsskr.22.0627. Print 2022 Oct 25. Tidsskr Nor Laegeforen. 2022. PMID: 36286563 Norwegian. No abstract available.
References
-
- Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, Woolf A, Vos T, Buchbinder R, A systematic review of the global prevalence of low back pain. Arthritis Rheum 64, 2028–2037 (2012). - PubMed
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators, Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 392, 1789–1858 (2018). - PMC - PubMed
-
- Chou R, Deyo R, Friedly J, Skelly A, Weimer M, Fu R, Dana T, Kraegel P, Griffin J, Grusing S, Systemic pharmacologic therapies for low back pain: A systematic review for an American College of Physicians clinical practice guideline. Ann. Intern. Med 166, 480–492 (2017). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
