

The crosstalk between bone remodeling and energy metabolism: A translational perspective
- PMID: 35545088
- PMCID: PMC9535690
- DOI: 10.1016/j.cmet.2022.04.010
The crosstalk between bone remodeling and energy metabolism: A translational perspective
Abstract
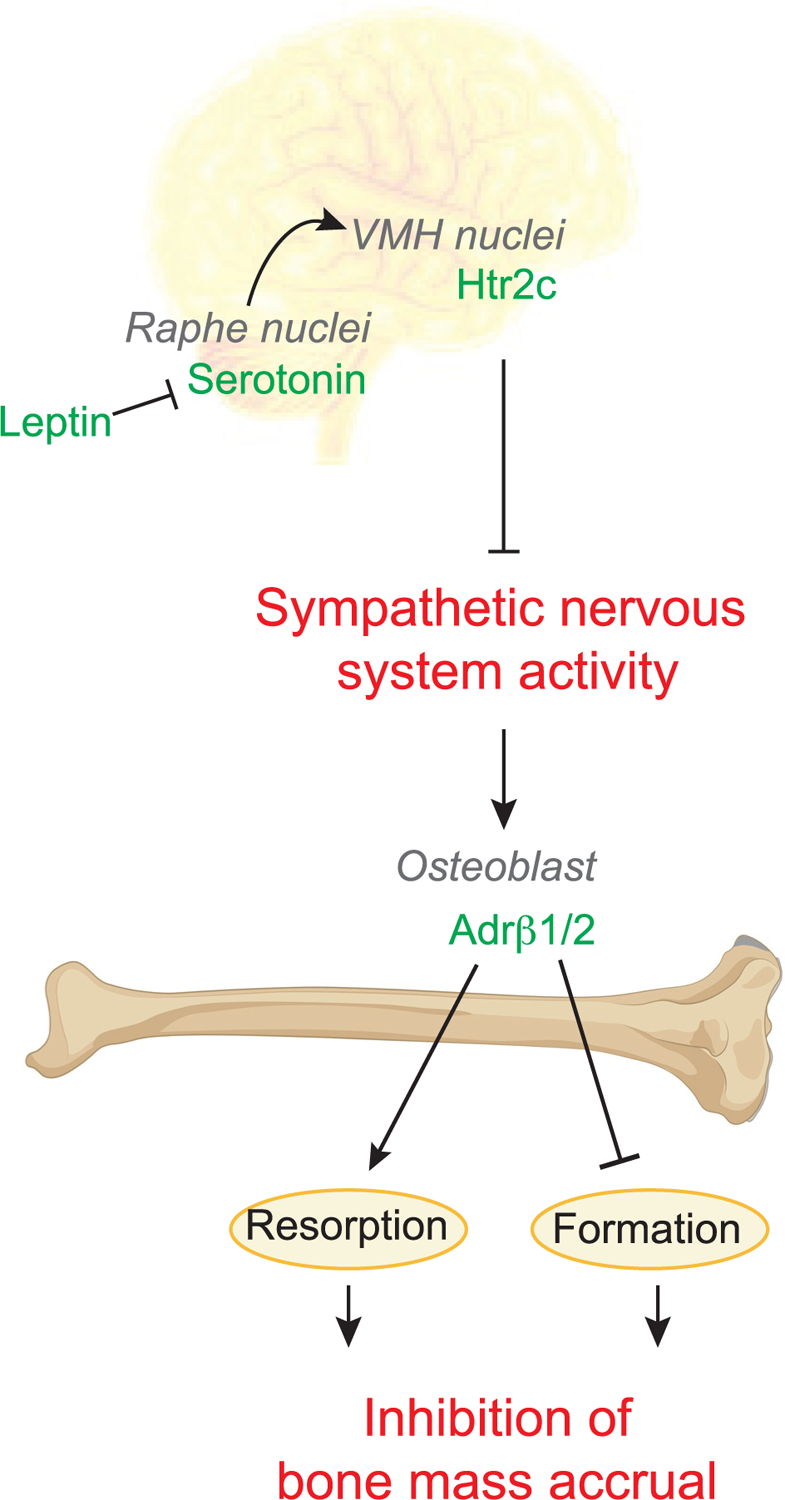
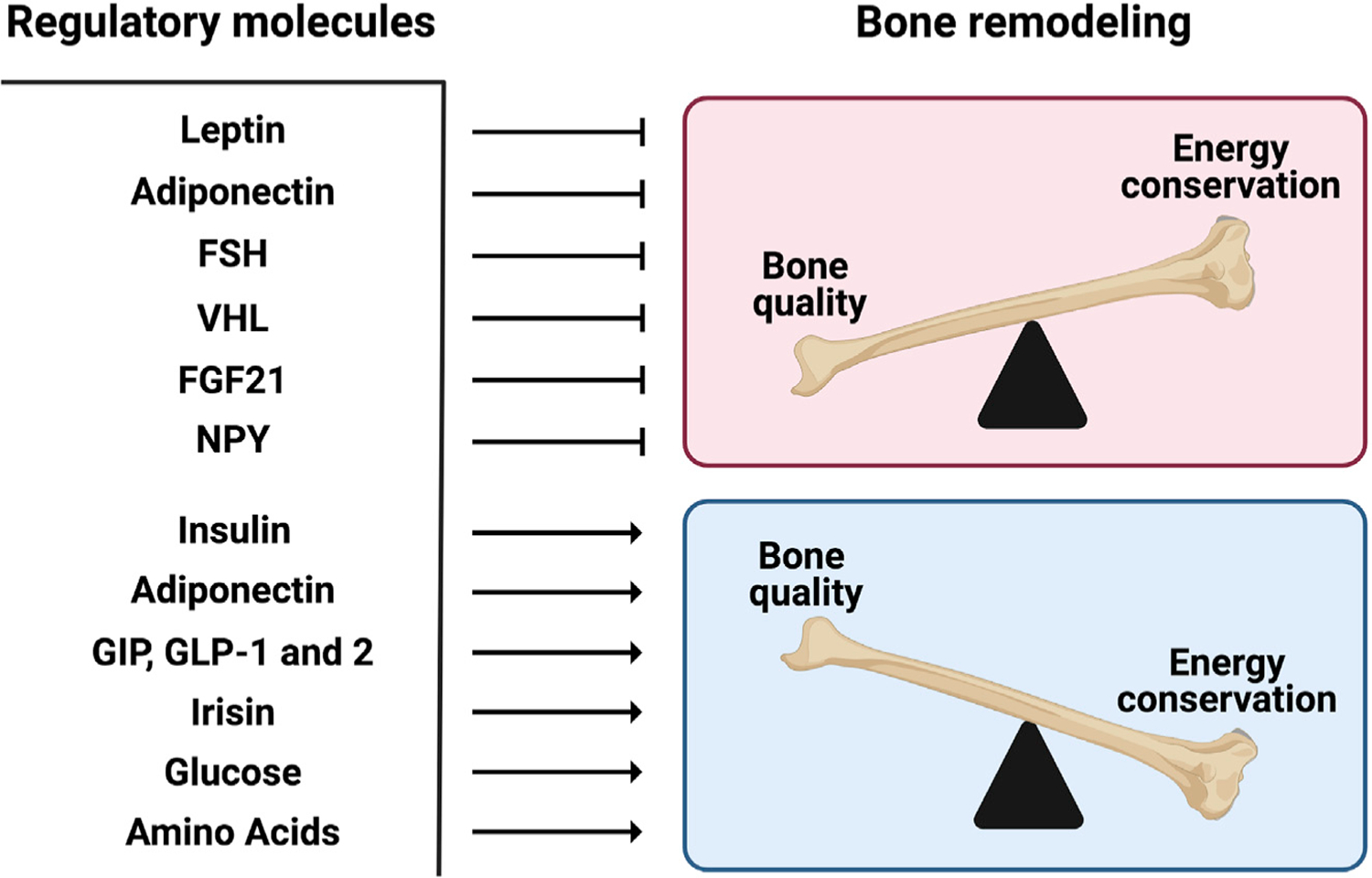
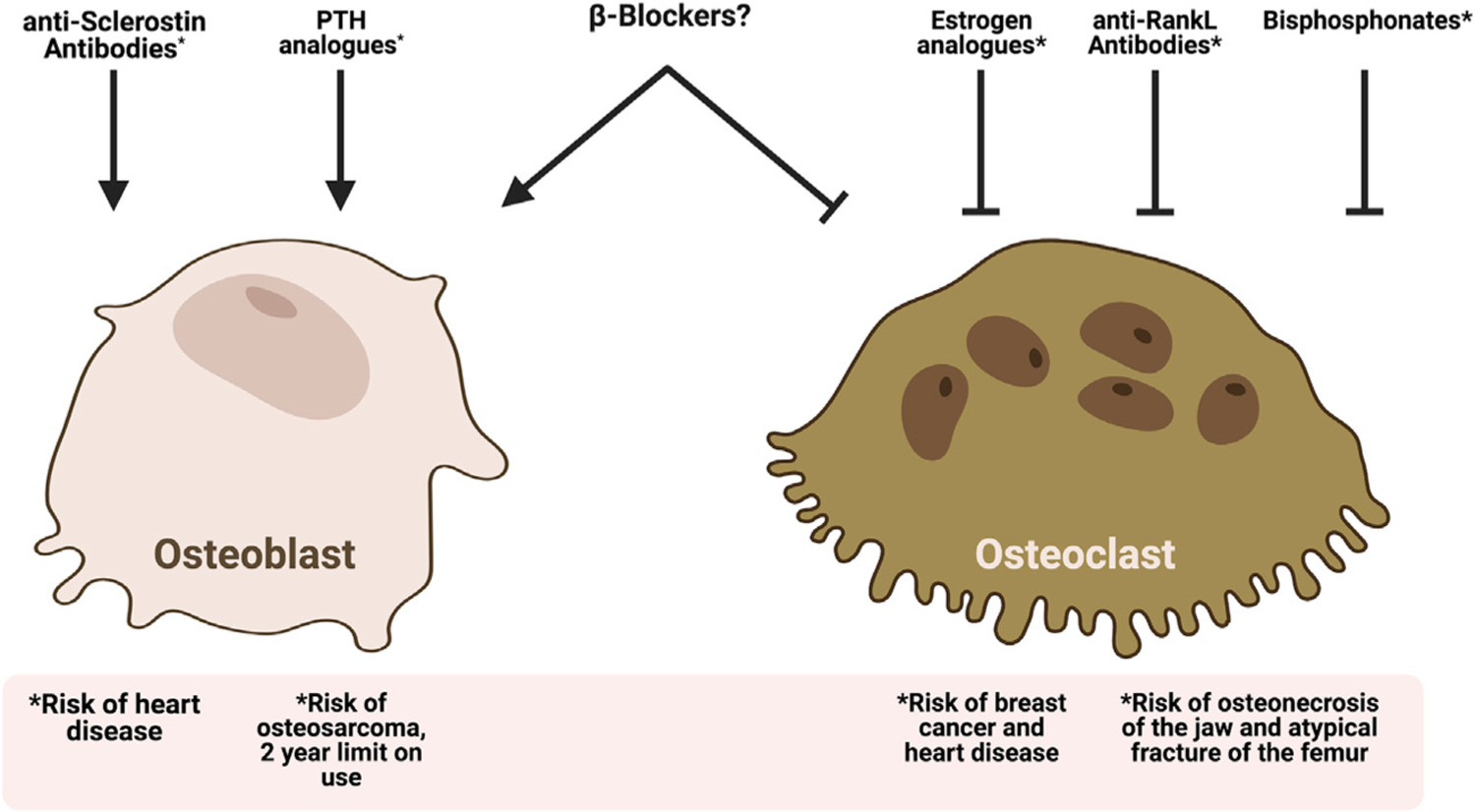
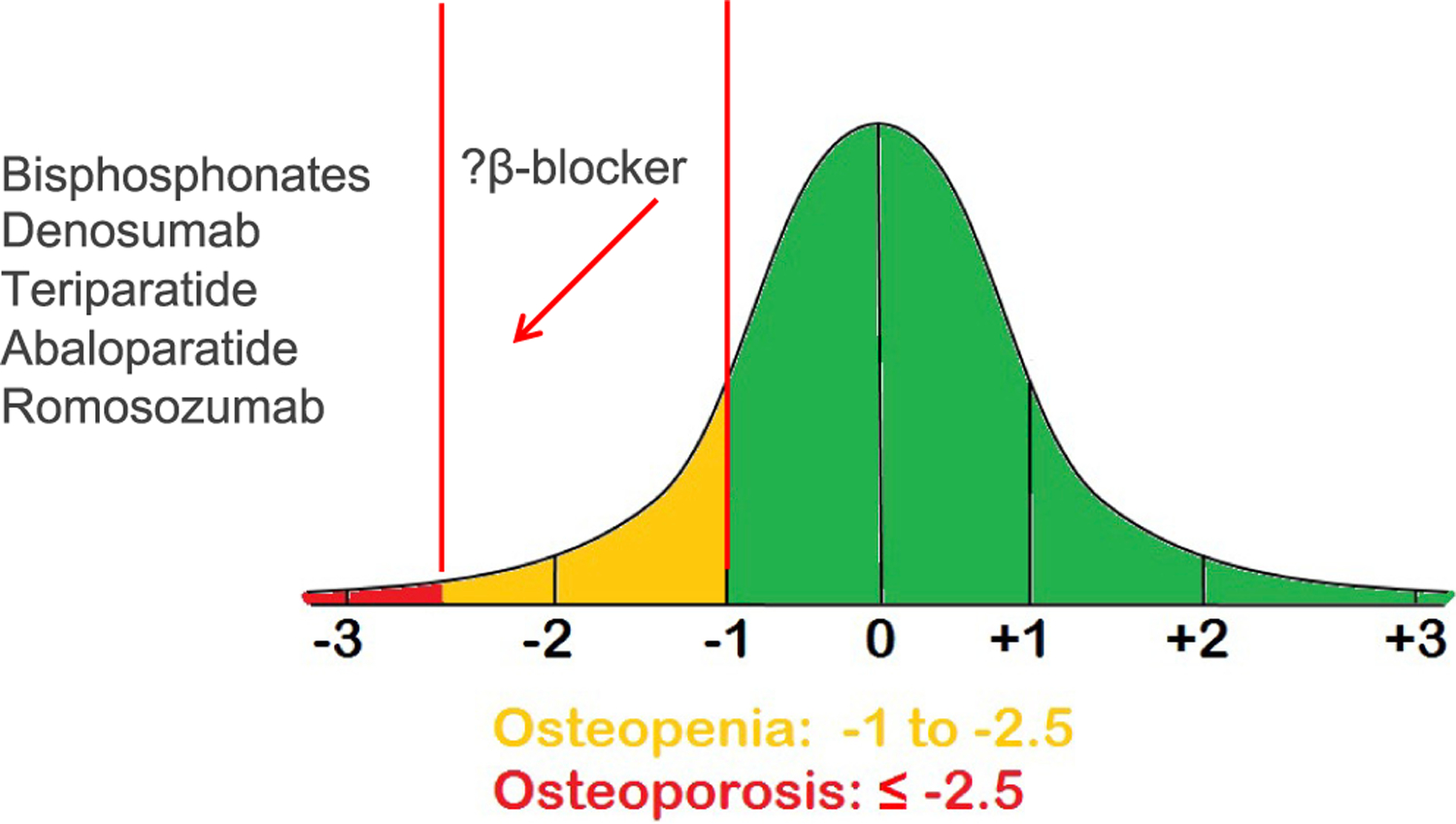
Genetics in model organisms has progressively broken down walls that previously separated different disciplines of biology. One example of this holistic evolution is the recognition of the complex relationship that exists between the control of bone mass (bone remodeling) and energy metabolism in mammals. Numerous hormones orchestrate this crosstalk. In particular, the study of the leptin-mediated regulation of bone mass has not only revealed the existence of a central control of bone mass but has also led to the realization that sympathetic innervation is a major regulator of bone remodeling. This happened at a time when the use of drugs aiming at treating osteoporosis, the most frequent bone disease, has dwindled. This review will highlight the main aspects of the leptin-mediated regulation of bone mass and how this led to the realization that β-blockers, which block the effects of the sympathetic nervous system, may be a viable option to prevent osteoporosis.
Keywords: coordinated regulation of bone mass and energy metabolism; osteoporosis; sympathetic regulation of bone mass; β-blockers.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures
References
-
- Ahn JD, Dubern B, Lubrano-Berthelier C, Clement K, and Karsenty G (2006). Cart overexpression is the only identifiable cause of high bone mass in melanocortin 4 receptor deficiency. Endocrinology 147, 3196–3202. - PubMed
-
- Ala M, Jafari RM, and Dehpour AR (2020). Diabetes mellitus and osteoporosis correlation: challenges and hopes. Curr. Diabetes Rev 16, 984–1001. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
