

Increased Reach and Effectiveness With a Low-Burden Point-of-Care Tobacco Treatment Program in Cancer Clinics
- PMID: 35545172
- PMCID: PMC9173433
- DOI: 10.6004/jnccn.2021.7333
Increased Reach and Effectiveness With a Low-Burden Point-of-Care Tobacco Treatment Program in Cancer Clinics
Abstract
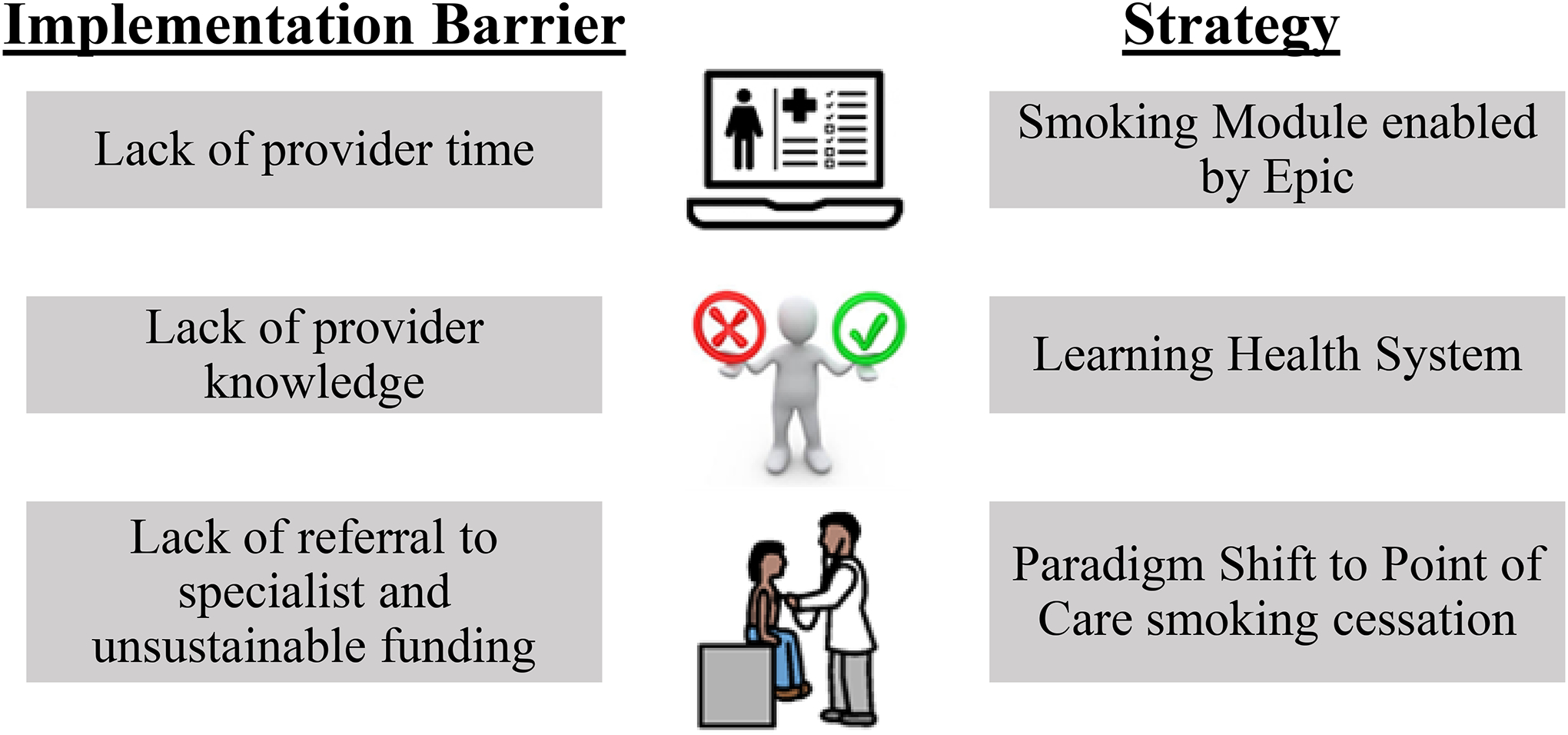
Background: Tobacco cessation after a cancer diagnosis can extend patient survival by improving outcomes for primary cancer and preventing secondary cancers. However, smoking is often unaddressed in cancer care, highlighting the need for strategies to increase treatment reach and cessation. This study examined a low-burden, point-of-care tobacco treatment program (ELEVATE) featuring an electronic health record-enabled smoking module and decision support tools to increase the reach and effectiveness of evidence-based smoking cessation treatment.
Methods: This study included adult outpatient tobacco smokers (n=13,651) in medical oncology, internal medicine, and surgical oncology clinics from a large midwestern healthcare system. We examined reach and effectiveness of ELEVATE with 2 comparisons: (1) preimplementation versus postimplementation of ELEVATE and (2) ELEVATE versus usual care. Data were evaluated during 2 time periods: preimplementation (January through May 2018) and postimplementation (June through December 2018), with smoking cessation assessed at the last follow-up outpatient encounter during the 6 months after these periods.
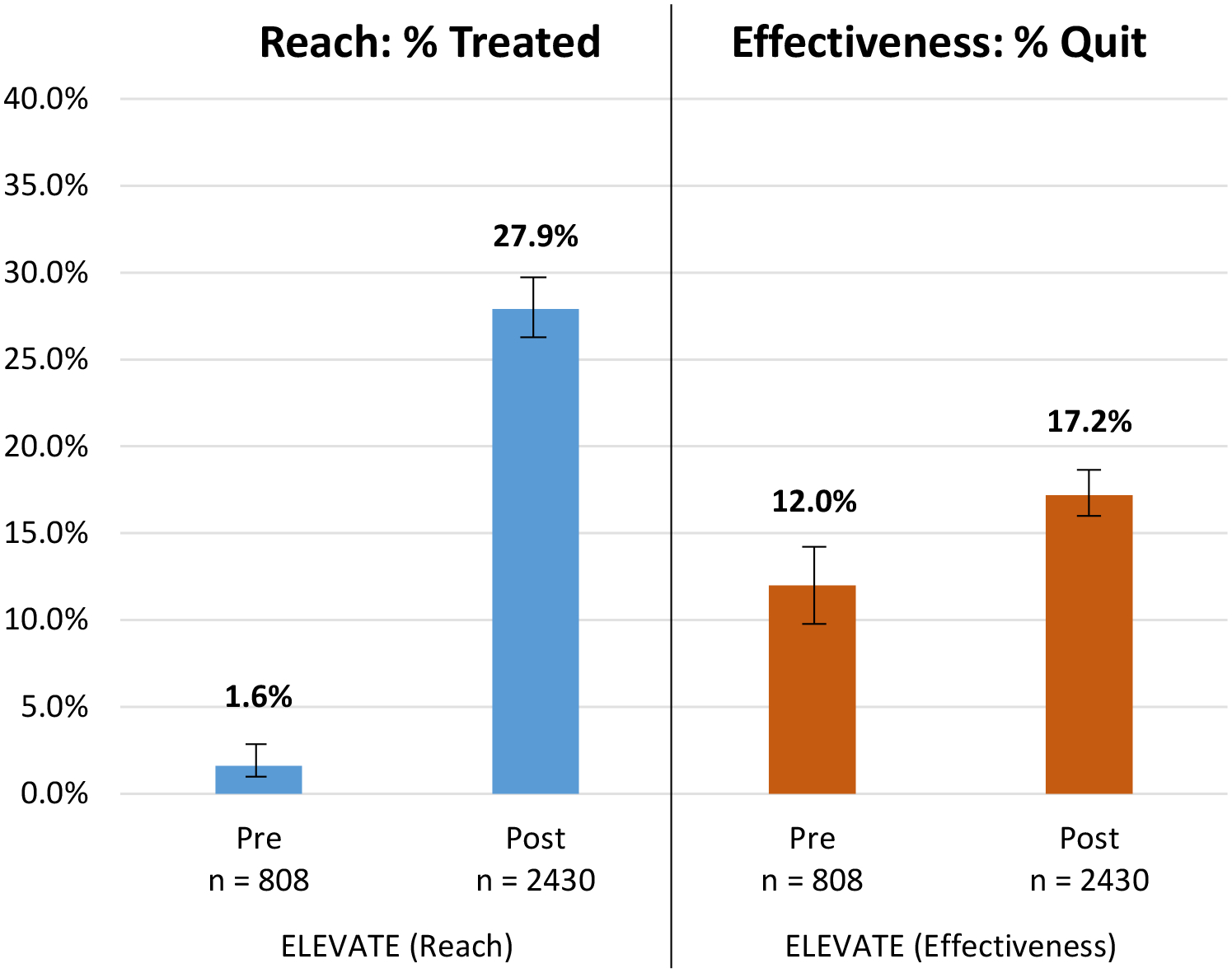
Results: The proportion of current tobacco smokers receiving cessation treatment increased from pre-ELEVATE to post-ELEVATE (1.6%-27.9%; difference, 26.3%; relative risk, 16.9 [95% CI, 9.8-29.2]; P<.001). Compared with 27.9% treatment reach with ELEVATE in the postimplementation time period, reach within usual care clinics ranged from 11.8% to 12.0% during this same period. The proportion of tobacco smokers who subsequently achieved cessation increased significantly from pre-ELEVATE to post-ELEVATE (12.0% vs 17.2%; difference, 5.2%; relative risk, 1.3 [95% CI, 1.1-1.5]; P=.002). Compared with 17.2% smoking cessation with ELEVATE in the postimplementation time period, achievement of cessation within usual care clinics ranged from 8.2% to 9.9% during this same period.
Conclusions: A low-burden, point-of-care tobacco treatment strategy increased tobacco treatment and cessation, thereby improving access to and the impact of evidence-based cessation treatment. Using implementation strategies to embed tobacco treatment in every healthcare encounter promises to engage more smokers in evidence-based treatment and facilitate smoking cessation, thereby improving care cancer for patients who smoke.
Figures
References
-
- CDC. Tobacco and Cancer: Centers for Disease Control and Prevention; 2019. [updated 22 October 2019. Available from: https://www.cdc.gov/cancer/tobacco/index.htm.
-
- Lortet-Tieulent J, Goding Sauer A, Siegel RL, et al. State-Level Cancer Mortality Attributable to Cigarette Smoking in the United States. JAMA Internal Medicine. 2016;176(12):1792–8. - PubMed
-
- National Cancer Institute. Cancer Statistics: NIH; 2018. [updated 27 April 2018. Available from: https://www.cancer.gov/about-cancer/understanding/statistics.
-
- Hanagiri T, Sugio K, Mizukami M, et al. Significance of Smoking as a Postoperative Prognostic Factor in Patients with Non-small Cell Lung Cancer. Journal of Thoracic Oncology. 2008;3(10):1127–32. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
