

Multicomponent intervention to prevent mobility disability in frail older adults: randomised controlled trial (SPRINTT project)
- PMID: 35545258
- PMCID: PMC9092831
- DOI: 10.1136/bmj-2021-068788
Multicomponent intervention to prevent mobility disability in frail older adults: randomised controlled trial (SPRINTT project)
Abstract
Objective: To determine whether a multicomponent intervention based on physical activity with technological support and nutritional counselling prevents mobility disability in older adults with physical frailty and sarcopenia.
Design: Evaluator blinded, randomised controlled trial.
Setting: 16 clinical sites across 11 European countries, January 2016 to 31 October 2019.
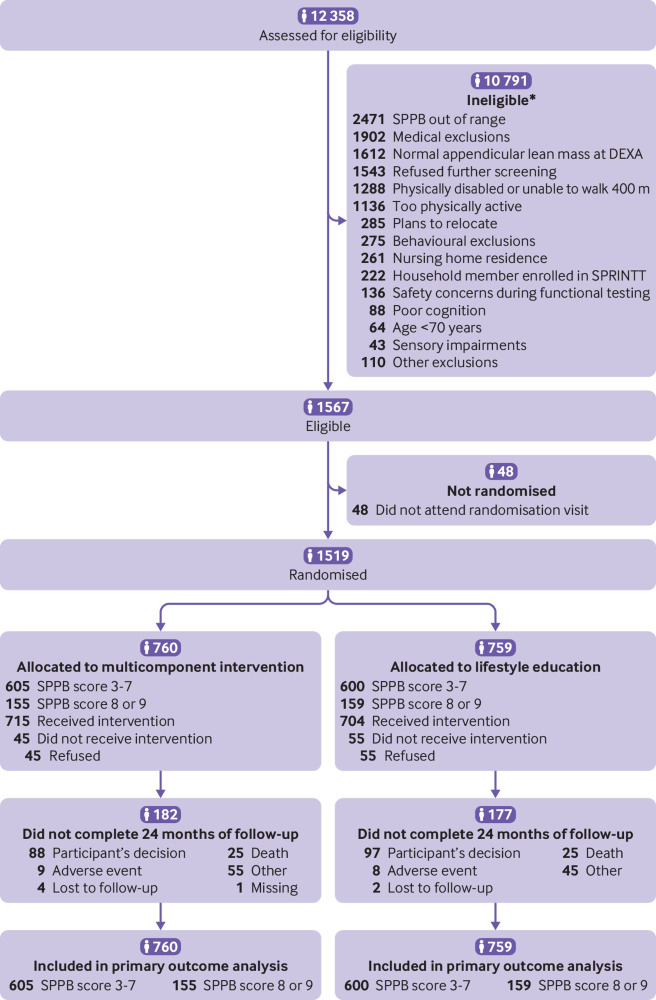
Participants: 1519 community dwelling men and women aged 70 years or older with physical frailty and sarcopenia, operationalised as the co-occurrence of low functional status, defined as a short physical performance battery (SPPB) score of 3 to 9, low appendicular lean mass, and ability to independently walk 400 m. 760 participants were randomised to a multicomponent intervention and 759 received education on healthy ageing (controls).
Interventions: The multicomponent intervention comprised moderate intensity physical activity twice weekly at a centre and up to four times weekly at home. Actimetry data were used to tailor the intervention. Participants also received personalised nutritional counselling. Control participants received education on healthy ageing once a month. Interventions and follow-up lasted for up to 36 months.
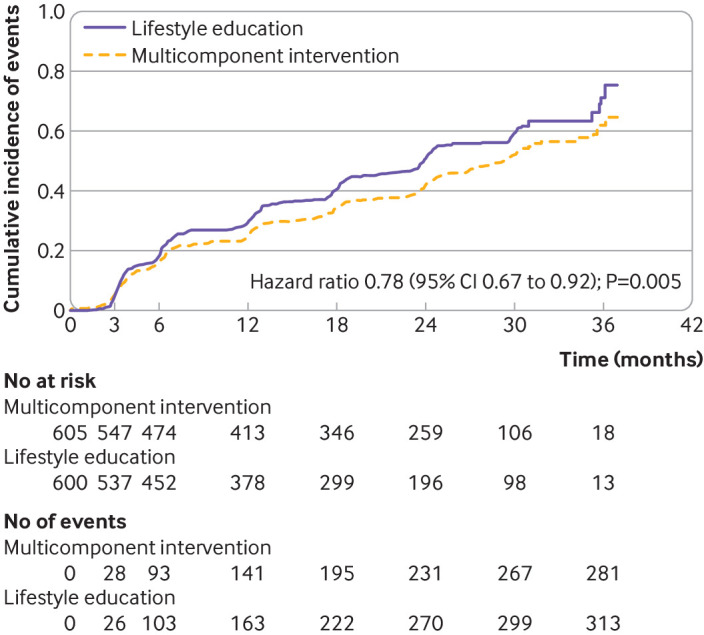
Main outcome measures: The primary outcome was mobility disability (inability to independently walk 400 m in <15 minutes). Persistent mobility disability (inability to walk 400 m on two consecutive occasions) and changes from baseline to 24 and 36 months in physical performance, muscle strength, and appendicular lean mass were analysed as pre-planned secondary outcomes. Primary comparisons were conducted in participants with baseline SPPB scores of 3-7 (n=1205). Those with SPPB scores of 8 or 9 (n=314) were analysed separately for exploratory purposes.
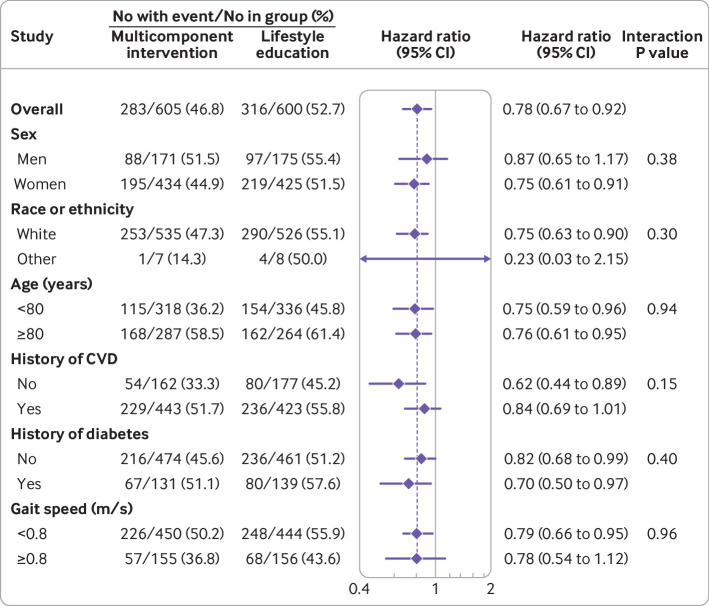
Results: Mean age of the 1519 participants (1088 women) was 78.9 (standard deviation 5.8) years. The average follow-up was 26.4 (SD 9.5) months. Among participants with SPPB scores of 3-7, mobility disability occurred in 283/605 (46.8%) assigned to the multicomponent intervention and 316/600 (52.7%) controls (hazard ratio 0.78, 95% confidence interval 0.67 to 0.92; P=0.005). Persistent mobility disability occurred in 127/605 (21.0%) participants assigned to the multicomponent intervention and 150/600 (25.0%) controls (0.79, 0.62 to 1.01; P=0.06). The between group difference in SPPB score was 0.8 points (95% confidence interval 0.5 to 1.1 points; P<0.001) and 1.0 point (95% confidence interval 0.5 to 1.6 points; P<0.001) in favour of the multicomponent intervention at 24 and 36 months, respectively. The decline in handgrip strength at 24 months was smaller in women assigned to the multicomponent intervention than to control (0.9 kg, 95% confidence interval 0.1 to 1.6 kg; P=0.028). Women in the multicomponent intervention arm lost 0.24 kg and 0.49 kg less appendicular lean mass than controls at 24 months (95% confidence interval 0.10 to 0.39 kg; P<0.001) and 36 months (0.26 to 0.73 kg; P<0.001), respectively. Serious adverse events occurred in 237/605 (39.2%) participants assigned to the multicomponent intervention and 216/600 (36.0%) controls (risk ratio 1.09, 95% confidence interval 0.94 to 1.26). In participants with SPPB scores of 8 or 9, mobility disability occurred in 46/155 (29.7%) in the multicomponent intervention and 38/159 (23.9%) controls (hazard ratio 1.25, 95% confidence interval 0.79 to 1.95; P=0.34).
Conclusions: A multicomponent intervention was associated with a reduction in the incidence of mobility disability in older adults with physical frailty and sarcopenia and SPPB scores of 3-7. Physical frailty and sarcopenia may be targeted to preserve mobility in vulnerable older people.
Trial registration: ClinicalTrials.gov NCT02582138.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: The present work was funded by a grant from the Innovative Medicines Initiative Joint Undertaking. AC, AJC-J, AJS, AMWJS, AS, AT, BV, CCS, EM, ET, FaL, FrL, IR, LM, LR-M, MC, MDB, MM, MT, PVJ, RB, RC, RR-W, SDA, SvH, and TS received in-kind support from the European Federation of Pharmaceutical Industries and Associations as part of the Innovative Medicines Initiative Joint Undertaking for the submitted work; CGA is a full time employee of Servier; HG, PB, and RaB are full time employees of Sanofi-Aventis; JS is a full time employee of Boehringer Ingelheim Pharma; MK is a full time employee of Astellas Pharma; RR and RRM are full time employees of Novartis; AJJ-C received grant support from Abbott Nutrition, Fresenius Kabi, and Nutricia outside of the submitted work, and personal fees from Abbott Nutrition, Fresenius Kabi, Nestlè, Nutricia, Pfizer, and Sanofi-Aventis outside of the submitted work; EM received personal fees from Abbott, Nestlè, Nutricia, and Thermofisher outside the submitted work; MC received personal fees from Nestlè outside the submitted work; RC received personal fees from Abbot and Nutricia outside the submitted work; SDA received grant support from Abbott and Vifor Pharma outside of the submitted work, and personal fees from Abbott, Bayer, Boehringer Ingelheim, Cardiac Dimension, Cordio, Impulse Dynamics, Novartis, Occlutech, Servier, and Vifor Pharma outside of the submitted work; SDS has a pending US patent; SvH received grant support from Amgen, Boehringer Ingelheim, and ZS Pharma outside of the submitted work and personal fees from AstraZeneca, Bayer, BRAHMS, Chugai, Grünenthal, Helsinn, Hexal, Merck Sharp and Dohme, Novartis, Pharmacosmos, Respicardia, Roche, Servier, and Sorin outside the submitted work; TF received personal fees from Bayer, BiosenseWebster, CSL Behring, Coherex Medical, Fresenius Kabi, Galapagos, Janssen, LivaNova, Minoryx, Novartis, Parexel, Penumbra, Roche, and Vifor Pharma outside the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Preserving community mobility in vulnerable older people.BMJ. 2022 May 11;377:o1084. doi: 10.1136/bmj.o1084. BMJ. 2022. PMID: 35545267 No abstract available.
-
In frail older adults with sarcopenia, a multicomponent intervention vs. education reduced mobility disability at 26 mo.Ann Intern Med. 2022 Sep;175(9):JC103. doi: 10.7326/J22-0062. Epub 2022 Sep 6. Ann Intern Med. 2022. PMID: 36063547
References
-
- Chen LK, Hwang AC, Lee WJ, et al. Taiwan Health Promotion Intervention Study for Elders research group . Efficacy of multidomain interventions to improve physical frailty, depression and cognition: data from cluster-randomized controlled trials. J Cachexia Sarcopenia Muscle 2020;11:650-62. 10.1002/jcsm.12534. - DOI - PMC - PubMed
-
- Innovative Medicines Initiative. 9th call for proposals 2013 – Innovative Medicines Initiative. July 2013. https://www.imi.europa.eu/sites/default/files/uploads/documents/apply-fo... (accessed 2 Mar 2022)
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical