

Outcome comparison of sural neurofasciocutaneous flap for reconstructing soft tissue defects in forefoot and around ankle
- PMID: 35545366
- PMCID: PMC10930481
- DOI: 10.11817/j.issn.1672-7347.2022.211227
Outcome comparison of sural neurofasciocutaneous flap for reconstructing soft tissue defects in forefoot and around ankle
Abstract
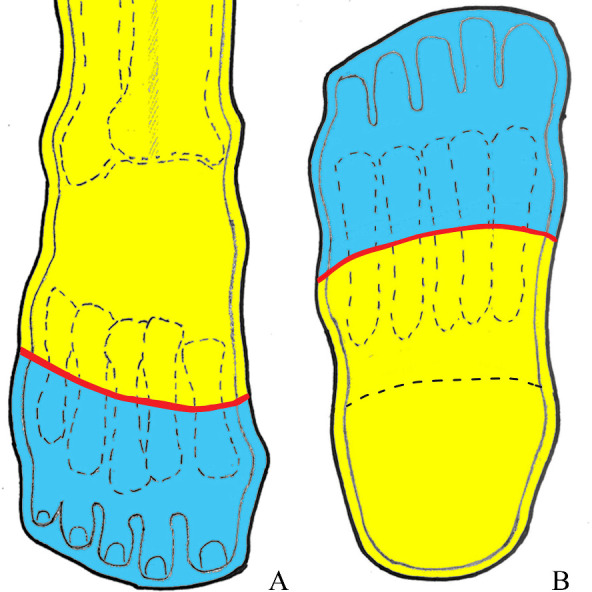
Objectives: To summarize our experience with the sural neurofasciocutaneous flap for reconstructing the soft tissue defects over the forefoot distal to the connecting line of midpoints in the metatarsal bones, and to compare the outcomes between the flap for resurfacing the defects distal and proximal to the connecting line.
Methods: The clinical data of 425 sural neurofasciocutaneous flaps for repairing the soft tissue defects in the middle and lower leg, ankle, and foot between Apr. 2002 and Apr. 2020 were reviewed. Based on the connecting line of midpoints of the metatarsals, the sural neurofasciocutaneous flaps were divided into a forefoot group (flaps with furthest edges distal to the connecting line) and a peri-ankle group (flaps with the furthest edges proximal to the connecting line).
Results: The partial necrosis rate in the forefoot group (14.5%, 10/69) was significantly higher than that in the peri-ankle group (7.0%, 25/356), with significant difference (P<0.05). Using the flap alone or in combination with a simple salvage treatment, the ratio of successful coverages of the defects was 98.6% (68/69) in the forefoot group, and 97.8% (348/356) in the peri-ankle group, respectively, with no statistical difference (P>0.05).
Conclusions: The sural neurofasciocutaneous flap is a better choice for covering the soft tissue defects over the forefoot distal to the connecting line of midpoints of the metatarsal bones. The survival reliability of the sural neurofasciocutaneous flap reconstructing the soft tissue defect proximal to the connecting line is superior to that of the flap reconstructing the defect distal to the connecting line.
目的: 总结腓肠神经营养血管皮瓣修复跖骨中点连线以远前足创面的临床经验,比较该皮瓣修复跖骨中点连线以远及以近创面的临床疗效。方法: 回顾性分析2002年4月至2020年4月间修复小腿中下段、踝及足部皮肤软组织缺损的425例腓肠神经营养血管皮瓣的临床资料。以跖骨中点连线为界,将腓肠神经营养血管皮瓣分为前足组(皮瓣最远端位于该连线以远的皮瓣)和踝周组(皮瓣最远端位于该连线以近的皮瓣)。结果: 前足组皮瓣部分坏死率(14.5%,10/69)高于踝周组(7.0%,25/356),两组比较差异有统计学意义(P<0.05)。前足组和踝周组单独应用该皮瓣或联合简单二期处理覆盖创面的成功率分别为98.6%(68/69)和97.8%(348/356),两组比较差异无统计学意义(P>0.05)。结论: 腓肠神经营养血管皮瓣是修复跖骨中点连线以远的前足皮肤软组织缺损的一种较理想的方法,该皮瓣修复跖骨中点连线以近创面的成活可靠性优于修复跖骨中点连线以远创面。.
Keywords: perforator flap; peroneal artery; sural nerve; surgical flap.
Conflict of interest statement
作者声称无任何利益冲突。
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
