

Physician adherence and patient-reported outcomes in heart failure with reduced ejection fraction in the era of angiotensin receptor-neprilysin inhibitor therapy
- PMID: 35545653
- PMCID: PMC9095619
- DOI: 10.1038/s41598-022-11740-5
Physician adherence and patient-reported outcomes in heart failure with reduced ejection fraction in the era of angiotensin receptor-neprilysin inhibitor therapy
Abstract
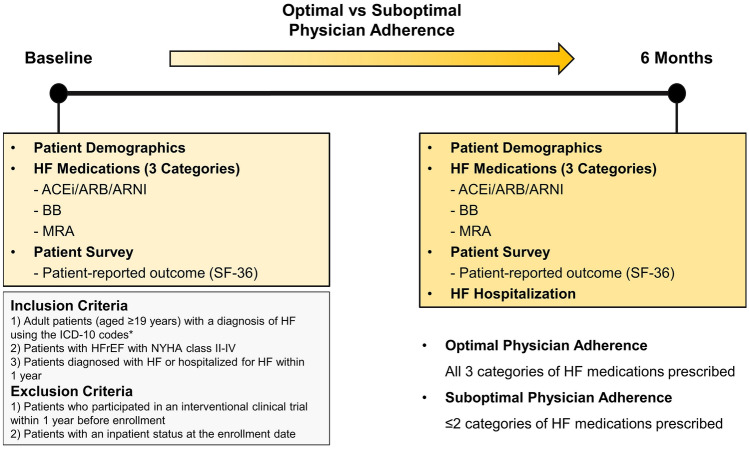
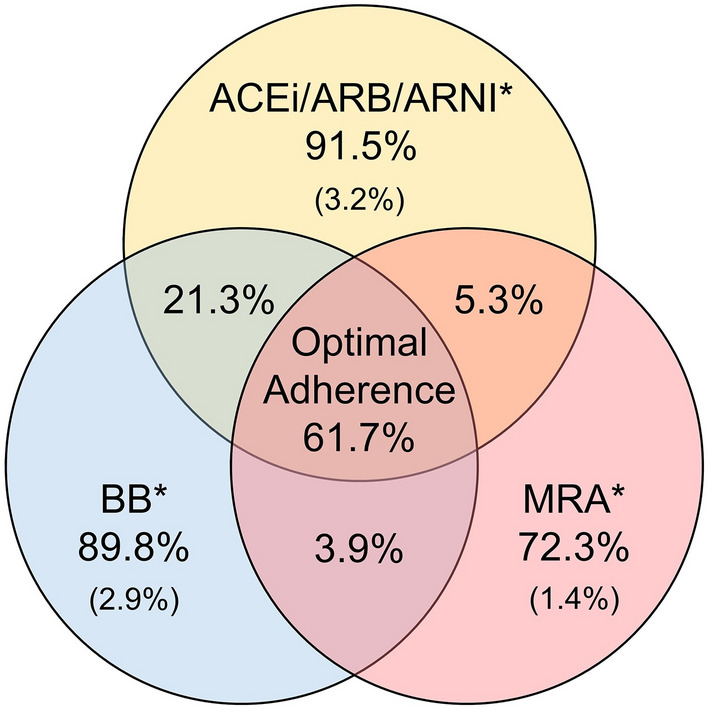
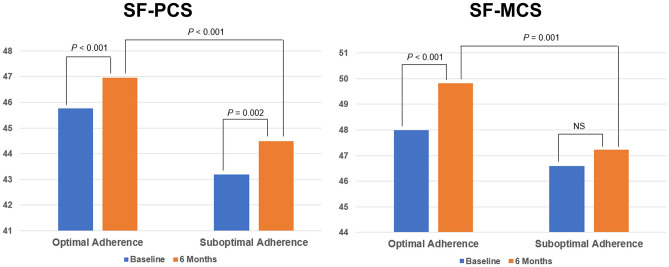
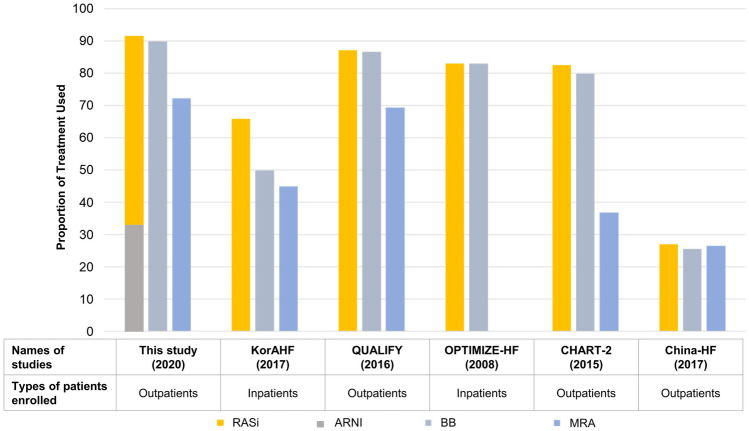
This Korean nationwide, multicenter, noninterventional, prospective cohort study aimed to analyze physician adherence to guideline-recommended therapy for heart failure (HF) with reduced ejection fraction (HFrEF) and its effect on patient-reported outcomes (PROs). Patients diagnosed with or hospitalized for HFrEF within the previous year were enrolled. Treatment adherence was considered optimal when all 3 categories of guideline-recommended medications (angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, or angiotensin receptor-neprilysin inhibitors; beta-blockers; and mineralocorticoid receptor antagonists) were prescribed and suboptimal when ≤ 2 categories were prescribed. The 36-Item Short Form Survey (SF-36) scores were compared at baseline and 6 months between the 2 groups. Overall, 854 patients from 30 hospitals were included. At baseline, the optimal adherence group comprised 527 patients (61.7%), whereas during follow-up, the optimal and suboptimal adherence groups comprised 462 (54.1%) and 281 (32.9%) patients, respectively. Patients in the suboptimal adherence group were older, with a lower body mass index, and increased comorbidities, including renal dysfunction. SF-36 scores were significantly higher in the optimal adherence group for most domains (P < 0.05). This study showed satisfactory physician adherence to contemporary treatment for HFrEF. Optimal adherence to HF medication significantly correlated with better PROs.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Kim ES, Youn JC, Baek SH. Update on the pharmacotherapy of heart failure with reduced ejection fraction. Cardiovasc. Prev. Pharmacother. 2020;2:113–133. doi: 10.36011/cpp.2020.2.e17. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
