

A combat casualty relevant dismounted complex blast injury model in swine
- PMID: 35545808
- PMCID: PMC9329201
- DOI: 10.1097/TA.0000000000003674
A combat casualty relevant dismounted complex blast injury model in swine
Abstract
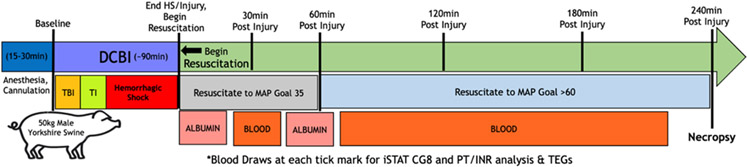
Background: Improvised explosive devices have resulted in a unique polytrauma injury pattern termed dismounted complex blast injury (DCBI), which is frequent in the modern military theater. Dismounted complex blast injury is characterized by extremity amputations, junctional vascular injury, and blast traumatic brain injury (bTBI). We developed a combat casualty relevant DCBI swine model, which combines hemorrhagic shock (HS) and tissue injury (TI) with a bTBI, to study interventions in this unique and devastating military injury pattern.
Methods: A 50-kg male Yorkshire swine were randomized to the DCBI or SHAM group (instrumentation only). Those in the DCBI group were subjected to HS, TI, and bTBI. The blast injury was applied using a 55-psi shock tube wave. Tissue injury was created with bilateral open femur fractures. Hemorrhagic shock was induced by bleeding from femoral arteries to target pressure. A resuscitation protocol modified from the Tactical Combat Casualty Care guidelines simulated battlefield resuscitation for 240 minutes.
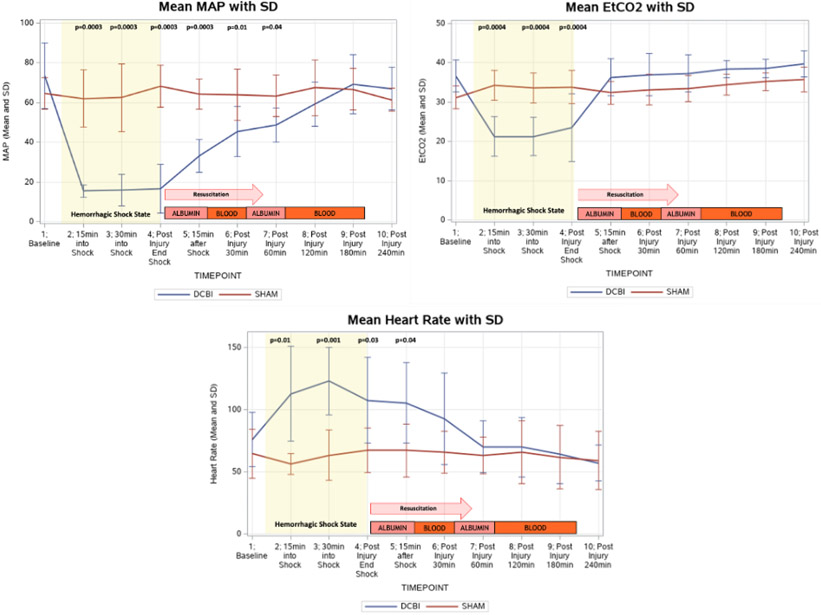
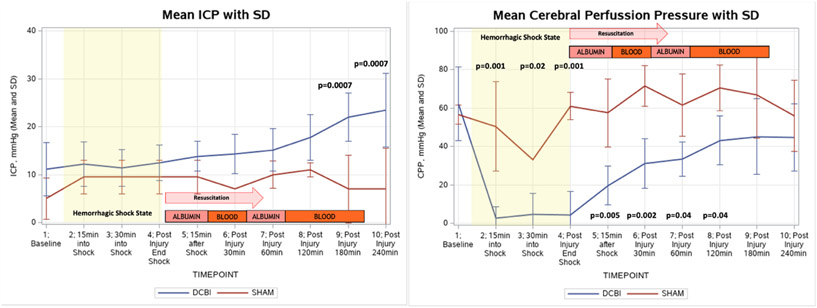
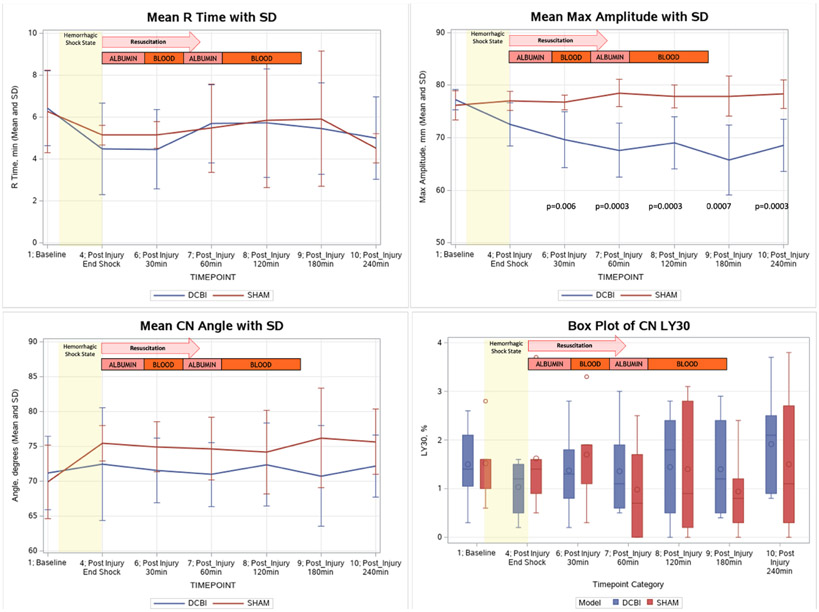
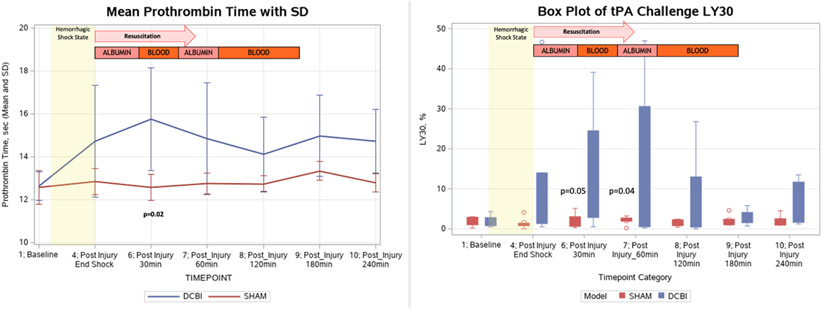
Results: Eight swine underwent the DCBI model and five were allocated to the SHAM group. In the DCBI model the mean base excess achieved at the end of the HS shock was -8.57 ± 5.13 mmol·L -1 . A significant coagulopathy was detected in the DCBI model as measured by prothrombin time (15.8 seconds DCBI vs. 12.86 seconds SHAM; p = 0.02) and thromboelastography maximum amplitude (68.5 mm DCBI vs. 78.3 mm in SHAM; p = 0.0003). For the DCBI models, intracranial pressure (ICP) increased by a mean of 13 mm Hg, reaching a final ICP of 24 ± 7.7 mm Hg.
Conclusion: We created a reproducible large animal model to study the combined effects of severe HS, TI, and bTBI on coagulation and ICP in the setting of DCBI, with significant translational applications for the care of military warfighters. Within the 4-hour observational period, the swine developed a consistent coagulopathy with a concurrent brain injury evidenced by increasing ICP.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Figures
References
-
- Cannon JW, Hofmann LJ, Glasgow SC, Potter BK, Rodriguez CJ, Cancio LC, et al. Dismounted Complex Blast Injuries: A Comprehensive Review of the Modern Combat Experience. J Am Coll Surg. Oct 2016;223(4):652–664 e658. - PubMed
-
- Eastridge BJ, Mabry RL, Seguin P, Cantrell J, Tops T, Uribe P, et al. Death on the battlefield (2001-2011): implications for the future of combat casualty care. J Trauma Acute Care Surg. Dec 2012;73(6 Suppl 5):S431–437. - PubMed
-
- Morrison JJ, Stannard A, Rasmussen TE, Jansen JO, Tai NR, Midwinter MJ. Injury pattern and mortality of noncompressible torso hemorrhage in UK combat casualties. J Trauma Acute Care Surg. Aug 2013;75(2 Suppl 2):S263–268. - PubMed
-
- Northern DM, Manley JD, Lyon R, Farber D, Mitchell BJ, Filak KJ, et al. Recent advances in austere combat surgery: Use of aortic balloon occlusion as well as blood challenges by special operations medical forces in recent combat operations. J Trauma Acute Care Surg. Jul 2018;85(1S Suppl 2):S98–S103. - PubMed
-
- Rees P. Response to: 'REBOA at Role 2 Afloat: resuscitative endovascular balloon occlusion of the aorta as a bridge to damage control surgery in the military maritime setting' by Rees et al. J R Army Med Corps. Jun 2019;165(3):213–214. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
