

Rehearsal simulation to determine the size of device for left atrial appendage occlusion using patient-specific 3D-printed phantoms
- PMID: 35546178
- PMCID: PMC9095622
- DOI: 10.1038/s41598-022-11967-2
Rehearsal simulation to determine the size of device for left atrial appendage occlusion using patient-specific 3D-printed phantoms
Abstract
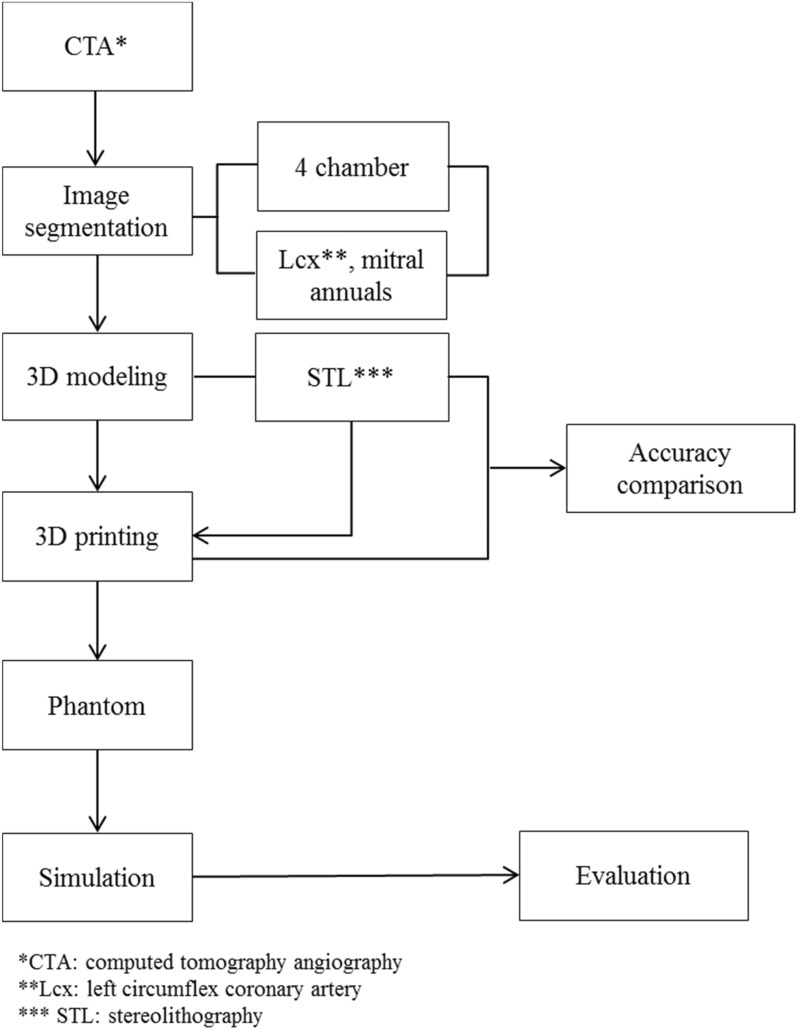
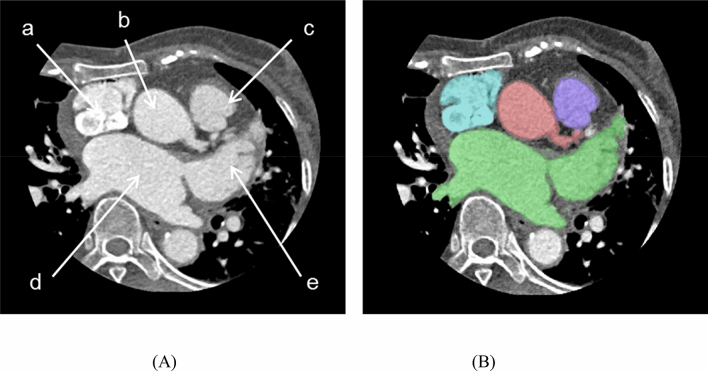
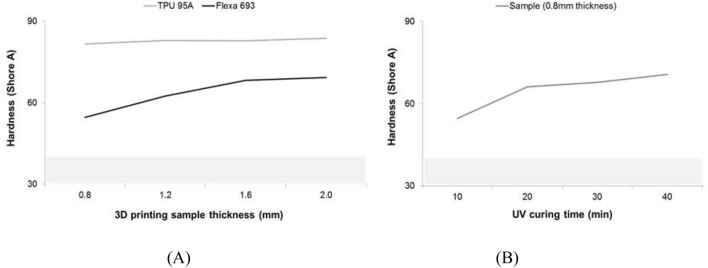
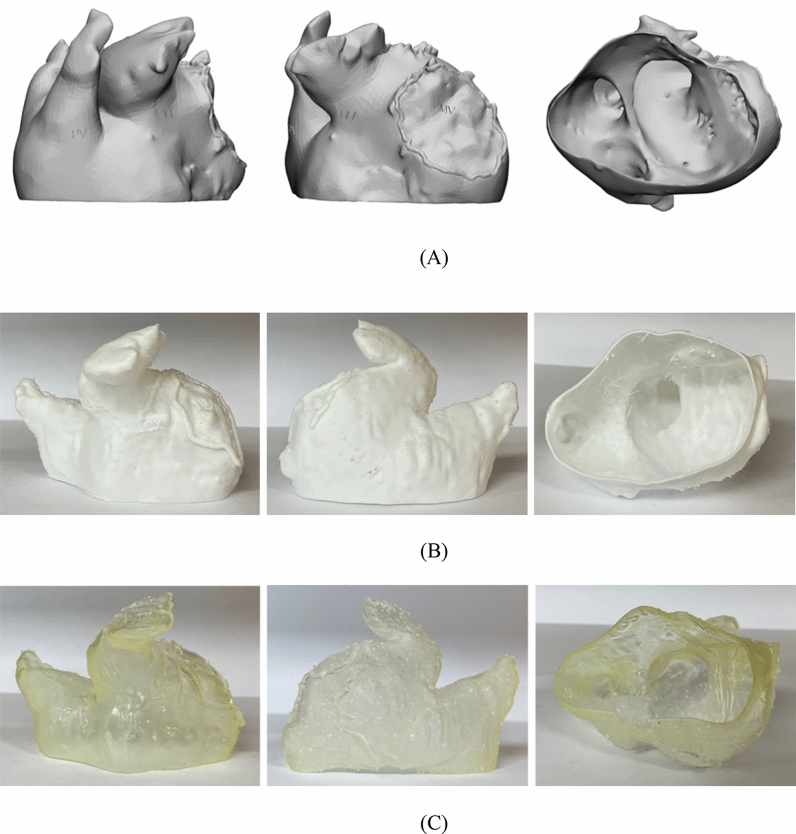
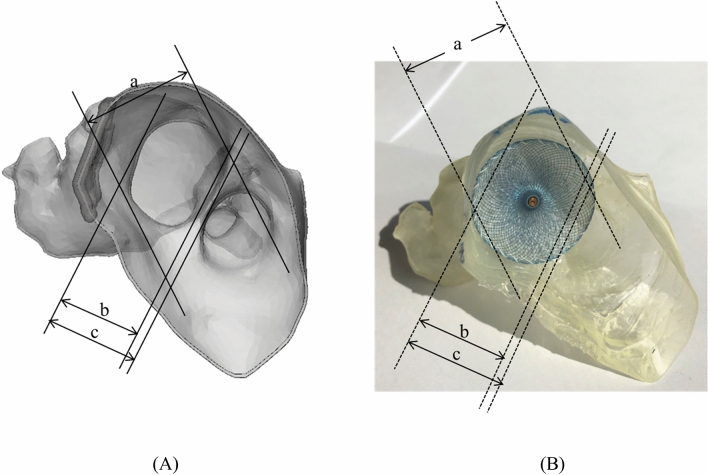
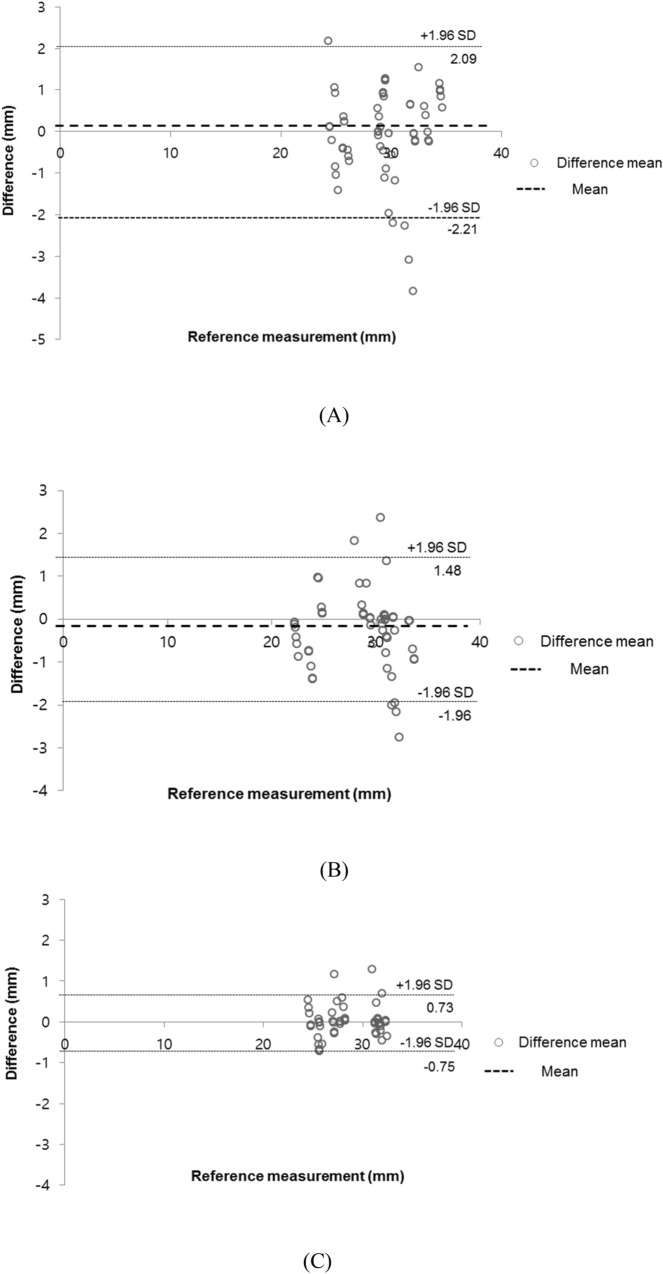
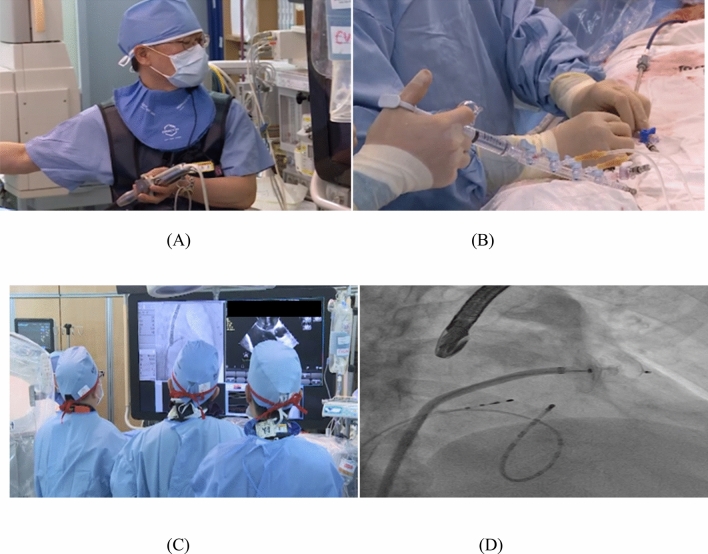
Left atrial appendage (LAA) occlusion (LAAO) is used to close the finger-like extension from the left atrium with occlusion devices to block the source of thrombosis. However, selection of the devices size is not easy due to various anatomical changes. The purpose of this study is patient-specific, computed tomography angiography (CTA)-based, three-dimensionally (3D) printed LAAO phantoms were applied pre-procedure to determine the size. Ten patients were enrolled prospectively in March 2019 and December 2020. The cardiac structure appearing in CTA was first segmented, and the left atrium and related structures in the LAAO procedure were modeled. The phantoms were fabricated using two methods of fused deposition modeling (FDM) and stereolithography (SLA) 3D printers with thermoplastic polyurethane (TPU) and flexible resin materials and evaluated by comparing their physical and material properties. The 3D-printed phantoms were directly used to confirm the shape of LAA, and to predict the device size for LAAO. In summary, the shore A hardness of TPU of FDM was about 80-85 shore A, and that of flexible resin of SLA was about 50-70 shore A. The measurement error between the STL model and 3D printing phantoms were 0.45 ± 0.37 mm (Bland-Altman, limits of agreement from - 1.8 to 1.6 mm). At the rehearsal, the estimations of device sizes were the exact same with those in the actual procedures of all 10 patients. In conclusion, simulation with a 3D-printed left atrium phantom could be used to predict the LAAO insertion device size accurately before the procedure.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Whitlock, R. P. Stroke and Left atrial appendage occlusion in cardiac surgery (2013).
-
- Briceno, D. F. et al. Left atrial appendage occlusion device and novel oral anticoagulants versus warfarin for stroke prevention in nonvalvular atrial fibrillation: systematic review and meta-analysis of randomized controlled trials. Circ. Arrhythmia Electrophysiol.8, 1057–1064 (2015). - PubMed
-
- Bayard YL, et al. PLAATO (Percutaneous Left Atrial Appendage Transcatheter Occlusion) for prevention of cardioembolic stroke in non-anticoagulation eligible atrial fibrillation patients: Results from the European PLAATO study. EuroIntervention. 2010;6:220–226. doi: 10.4244/EIJV6I2A35. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
