

Neurologic complications of infective endocarditis in children
- PMID: 35546418
- PMCID: PMC9652479
- DOI: 10.1017/S1047951122001159
Neurologic complications of infective endocarditis in children
Abstract
Objectives: To define the frequency and characteristics of acute neurologic complications in children hospitalised with infective endocarditis and to identify risk factors for neurologic complications.
Study design: Retrospective cohort study of children aged 0-18 years hospitalised at a tertiary children's hospital from 1 January, 2008 to 31 December, 2017 with infective endocarditis.
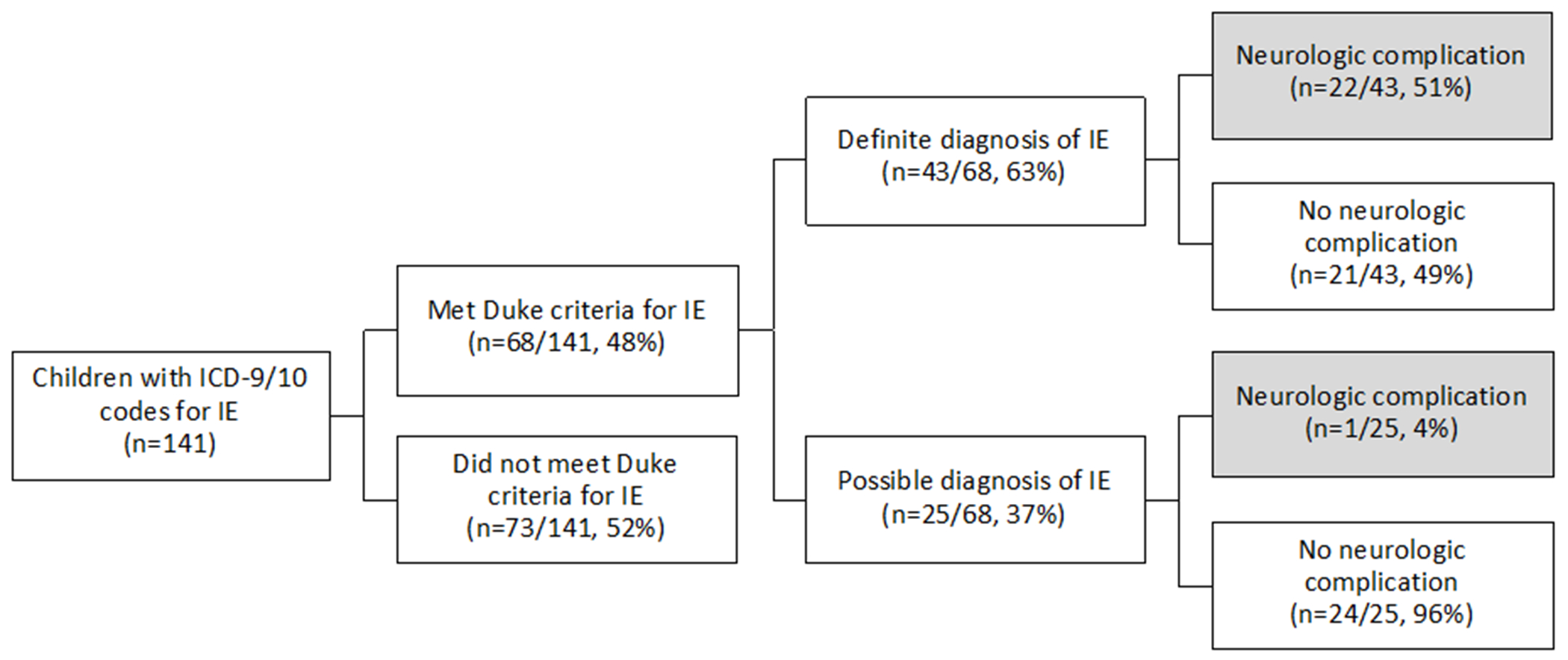
Results: Sixty-eight children met Duke criteria for infective endocarditis (43 definite and 25 possible). Twenty-three (34%) had identified neurologic complications, including intracranial haemorrhage (25%, 17/68) and ischaemic stroke (25%, 17/68). Neurologic symptoms began a median of 4.5 days after infective endocarditis symptom onset (interquartile range 1, 25 days), though five children were asymptomatic and diagnosed on screening neuroimaging only. Overall, only 56% (38/68) underwent neuroimaging during acute hospitalisation, so additional asymptomatic neurologic complications may have been missed. Children with identified neurologic complications compared to those without were older (48 versus 22% ≥ 13 years old, p = 0.031), more often had definite rather than possible infective endocarditis (96 versus 47%, p < 0.001), mobile vegetations >10mm (30 versus 11%, p = 0.048), and vegetations with the potential for systemic embolisation (65 versus 29%, p = 0.004). Six children died (9%), all of whom had neurologic complications.
Conclusions: Neurologic complications of infective endocarditis were common (34%) and associated with mortality. The true frequency of neurologic complications was likely higher because asymptomatic cases may have been missed without screening neuroimaging. Moving forward, we advocate that all children with infective endocarditis have neurologic consultation, examination, and screening neuroimaging. Additional prospective studies are needed to determine whether early identification of neurologic abnormalities may direct management and ultimately reduce neurologic morbidity and overall mortality.
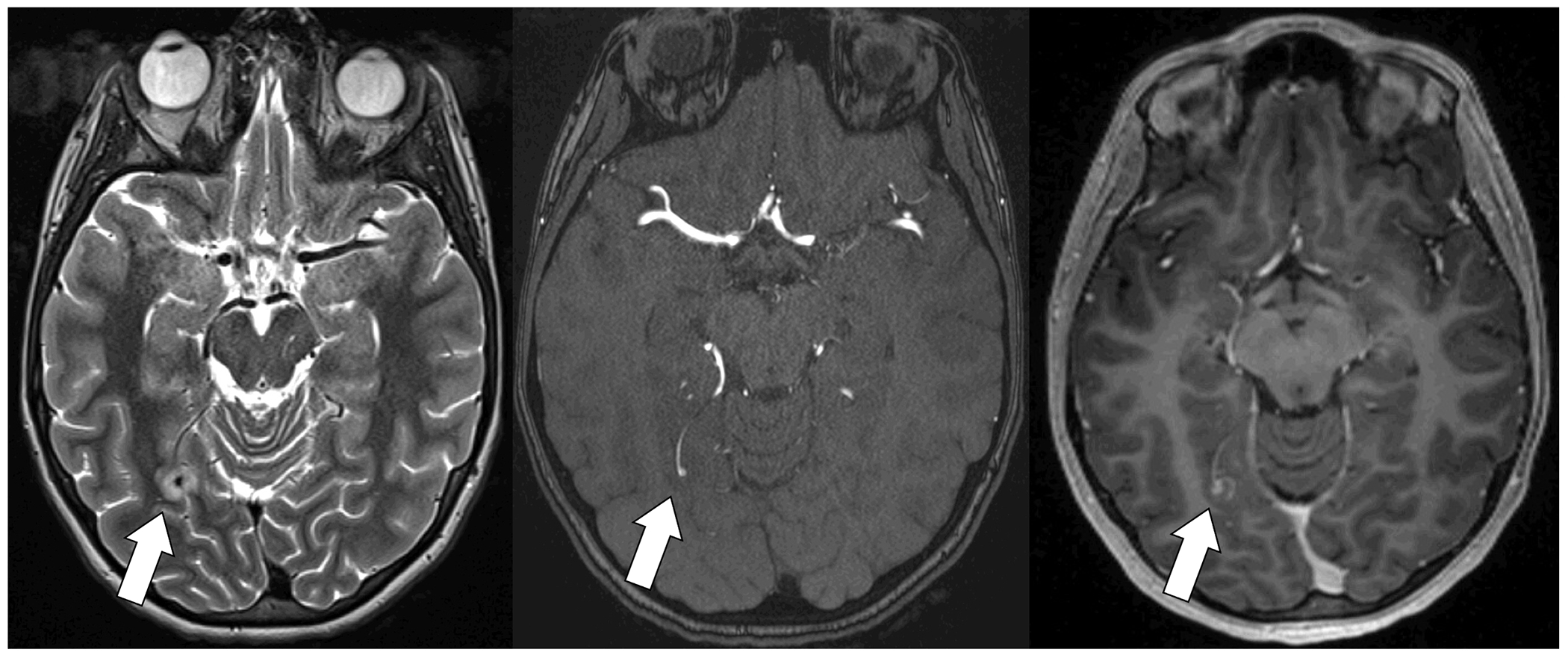
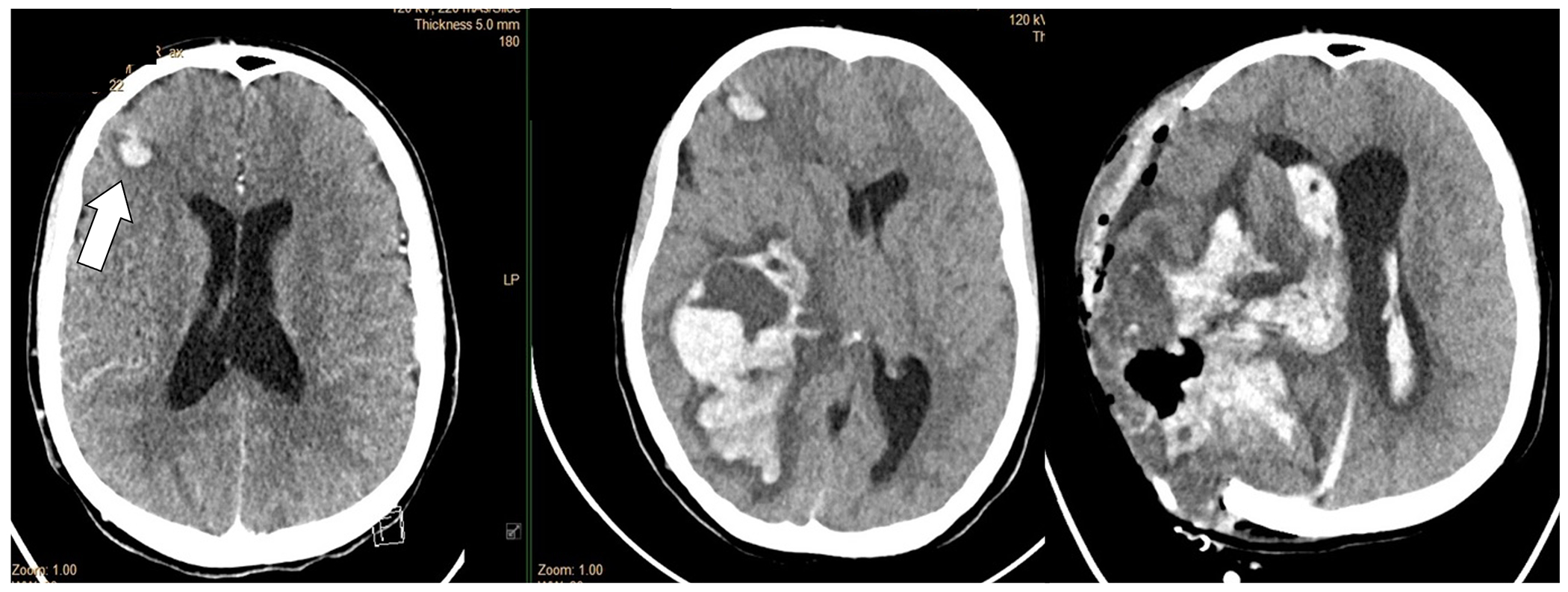
Keywords: CHD; Infective endocarditis; infectious intracranial aneurysm; intracranial haemorrhage; neuroimaging; stroke.
Conflict of interest statement
Figures
References
-
- Pasquali SK, He X, Mohamad Z, McCrindle BW, Newburger JW, Li JS, et al. Trends in endocarditis hospitalizations at US children’s hospitals: impact of the 2007 American Heart Association Antibiotic Prophylaxis Guidelines. Am Heart J. 2012;163(5):894–899. doi: 10.1016/j.ahj.2012.03.002 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
