

Evaluating alternative methods of comparing antihypertensive treatment intensity
- PMID: 35546588
- PMCID: PMC10694801
- DOI: 10.37765/ajmc.2022.89146
Evaluating alternative methods of comparing antihypertensive treatment intensity
Abstract
Objectives: To change blood pressure treatment, clinicians can modify medication count or dose. However, existing studies have measured count modification, which may miss clinically important dose change in the absence of count change. This research demonstrates how dose modification captures more information about management than medication count alone.
Study design: Retrospective cohort study.
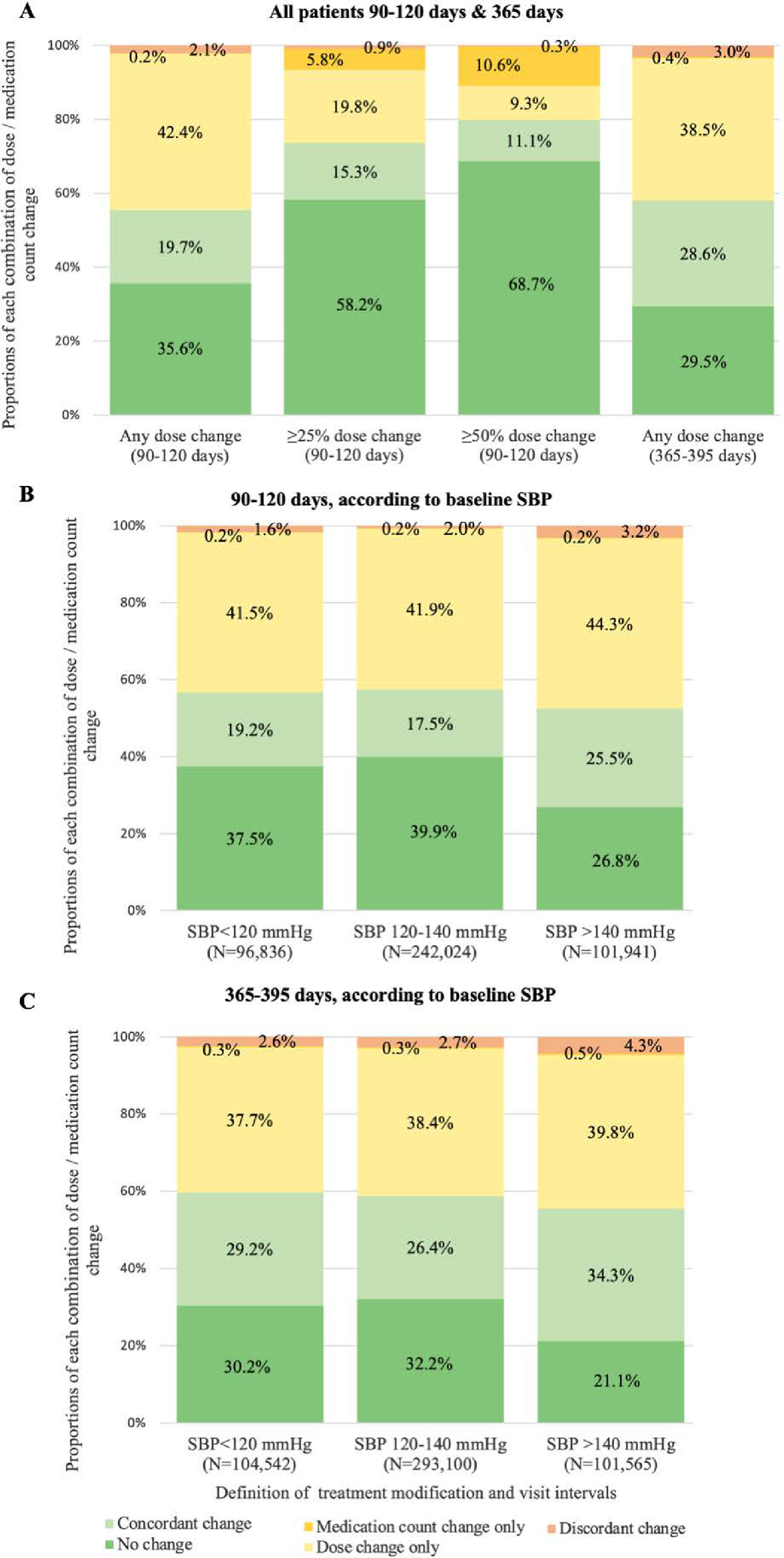
Methods: We included patients 65 years and older with established primary care at the Veterans Health Administration (July 2011-June 2013). We captured medication count and standardized dose change over 90 to 120 days using a validated pharmacy fill algorithm. We determined frequency of dose change without count change (and vice versa), no change in either, change in same direction ("concordant"), and change in opposite direction ("discordant"). We compared change according to systolic blood pressure (SBP) and compared concordance using a minimum threshold definition of dose change of at least 50% (instead of any change) of baseline dose modification.
Results: Among 440,801 patients, 64.2% had dose change; 22.0%, count change; 35.6%, no change in either; 42.4%, dose change without count modification; and 0.2%, count change without dose modification. Discordance occurred in 2.1% of observations. Using the minimum threshold definition of change, 68.7% had no change in either dose or count. Treatment was more frequently changed at SBP greater than 140 mm Hg.
Conclusions: Measuring change in antihypertensive treatment using medication count frequently missed an isolated dose change in treatment modification and less often misclassified regimen modifications where there was no modification in total dose. In future research, measuring dose modification using our new algorithm would capture change in hypertension treatment intensity more precisely than current methods.
Conflict of interest statement
DECLARATIONS
Figures
References
-
- Onder G, van der Cammen TJ, Petrovic M, Somers A, Rajkumar C. Strategies to reduce the risk of iatrogenic illness in complex older adults. Age Ageing. 2013;42(3):284–291. - PubMed
-
- Gueyffier F, Bulpitt C, Boissel JP, et al. Antihypertensive drugs in very old people: a subgroup meta-analysis of randomised controlled trials. INDANA Group. Lancet. 1999;353(9155):793–796. - PubMed
-
- Staessen JA, Gasowski J, Wang JG, et al. Risks of untreated and treated isolated systolic hypertension in the elderly: meta-analysis of outcome trials. Lancet. 2000;355(9207):865–872. - PubMed
-
- Beckett NS, Peters R, Fletcher AE, et al. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358(18):1887–1898. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
