

Prolonged casualty care: Extrapolating civilian data to the military context
- PMID: 35546736
- PMCID: PMC9323558
- DOI: 10.1097/TA.0000000000003675
Prolonged casualty care: Extrapolating civilian data to the military context
Abstract
Background: Civilian and military populations alike are increasingly faced with undesirable situations in which prehospital and definitive care times will be delayed. The Western Cape of South Africa has some similarities in capabilities, injury profiles, resource limitations, and system configuration to US military prolonged casualty care (PCC) settings. This study provides an initial description of civilians in the Western Cape who experience PCC and compares the PCC and non-PCC populations.
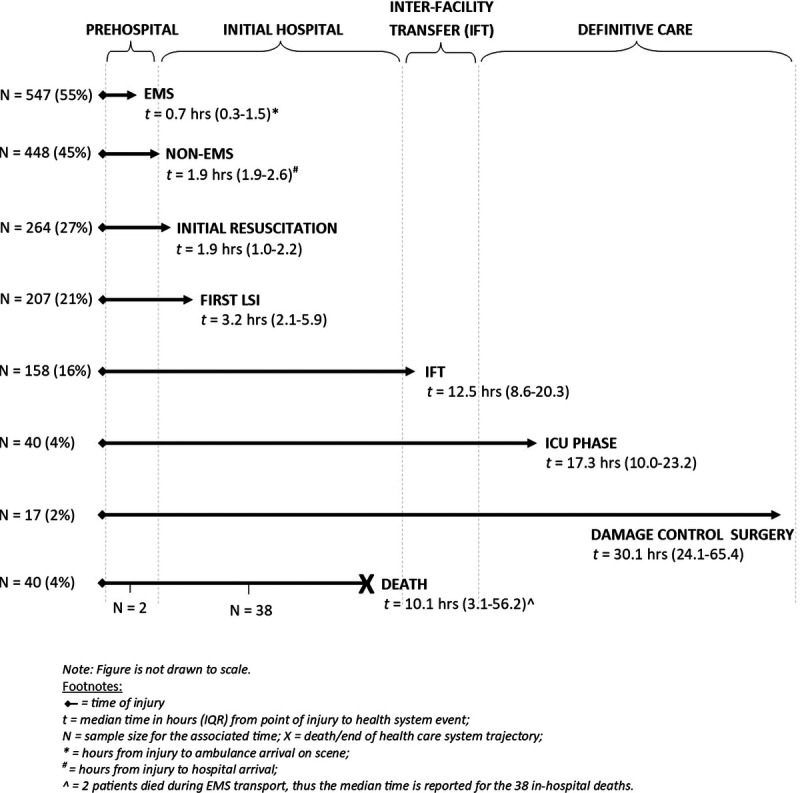
Methods: We conducted a 6-month analysis of an ongoing, prospective, large-scale epidemiologic study of prolonged trauma care in the Western Cape (Epidemiology and Outcomes of Prolonged Trauma Care [EpiC]). We define PCC as ≥10 hours from injury to arrival at definitive care. We describe patient characteristics, critical interventions, key times, and outcomes as they may relate to military PCC and compare these using χ 2 and Wilcoxon tests. We estimated the associations between PCC status and the primary and secondary outcomes using logistic regression models.
Results: Of 995 patients, 146 experienced PCC. The PCC group, compared with non-PCC, were more critically injured (66% vs. 51%), received more critical interventions (36% vs. 29%), and had a greater proportionate mortality (5% vs. 3%), longer hospital stays (3 vs. 1 day), and higher Sequential Organ Failure Assessment scores (5 vs. 3). The odds of 7-day mortality and a Sequential Organ Failure Assessment score of ≥5 were 1.6 (odds ratio, 1.59; 95% confidence interval, 0.68-3.74) and 3.6 (odds ratio, 3.69; 95% confidence interval, 2.11-6.42) times higher, respectively, in PCC versus non-PCC patients.
Conclusion: The EpiC study enrolled critically injured patients with PCC who received resuscitative interventions. Prolonged casualty care patients had worse outcomes than non-PCC. The EpiC study will be a useful platform to provide ongoing data for PCC relevant analyses, for future PCC-focused interventional studies, and to develop PCC protocols and algorithms. Findings will be relevant to the Western Cape, South Africa, other LMICs, and military populations experiencing prolonged care.
Level of evidence: Therapeutic/care management; Level IV.
Copyright © 2022 Written work prepared by employees of the Federal Government as part of their official duties is, under the U.S. Copyright Act, a “work of the United States Government” for which copyright protection under Title 17 of the United States Code is not available. As such, copyright does not extend to the contributions of employees of the Federal Government.
Figures


References
-
- Cohen AB, Davis M, Herman SEM. Prolonged field care research approach and its relevance to civilian medicine. Mil Med. 2021;186(5–6):123–128. - PubMed
-
- Keenan S, Riesberg JC. Prolonged field care: beyond the “golden hour”. Wilderness Environ Med. 2017;28(2S):S135–S139. - PubMed
-
- WHO . Guidelines for Essential Trauma Care 2004. Available at: https://www.who.int/violence_injury_prevention/publications/services/en/.... Accessed January 30, 2022.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
