

DyeVert Contrast Reduction System Use in Patients Undergoing Coronary and/or Peripheral Angiography: A Systematic Literature Review and Meta-Analysis
- PMID: 35547222
- PMCID: PMC9081570
- DOI: 10.3389/fmed.2022.841876
DyeVert Contrast Reduction System Use in Patients Undergoing Coronary and/or Peripheral Angiography: A Systematic Literature Review and Meta-Analysis
Abstract
Background: Contrast-associated acute kidney injury (CA-AKI) is an important adverse effect associated with injecting iodinated intra-arterial contrast media (CM) during coronary angiography. The DyeVert™ Contrast Reduction System is a medical device intended to reduce the intra-arterial CM volume (CMV) administered. The aim of this study was to assess DyeVert System clinical effectiveness and safety by implementing a systematic review and meta-analysis of existing evidence.
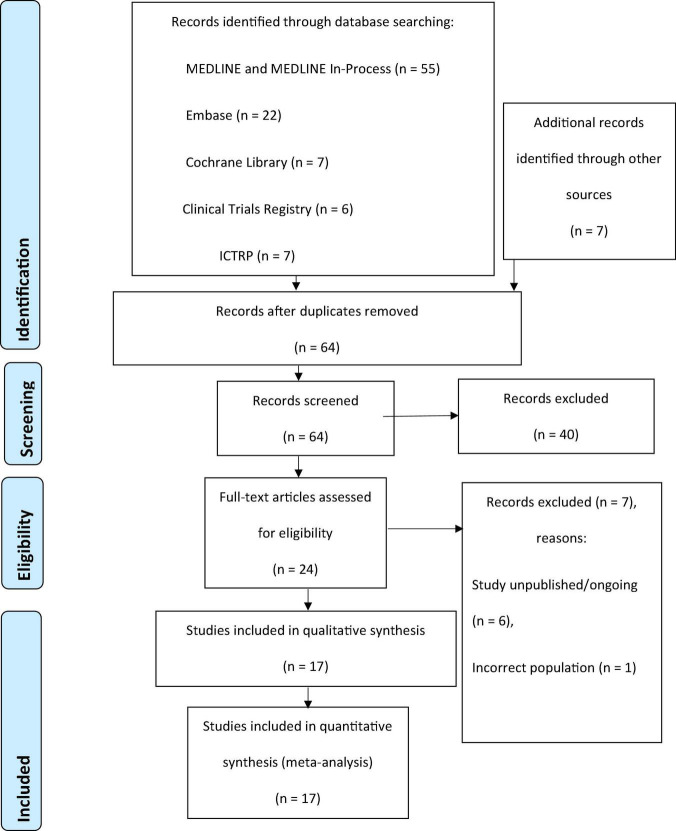
Methods: Systematic electronic literature searches were conducted in MEDLINE, Embase, the Cochrane Database of Systematic Reviews, ClinicalTrials.gov, and the International Clinical Trials Registry Platform database. Relevant data were extracted from included studies and meta-analyses were performed to synthesize evidence across studies.
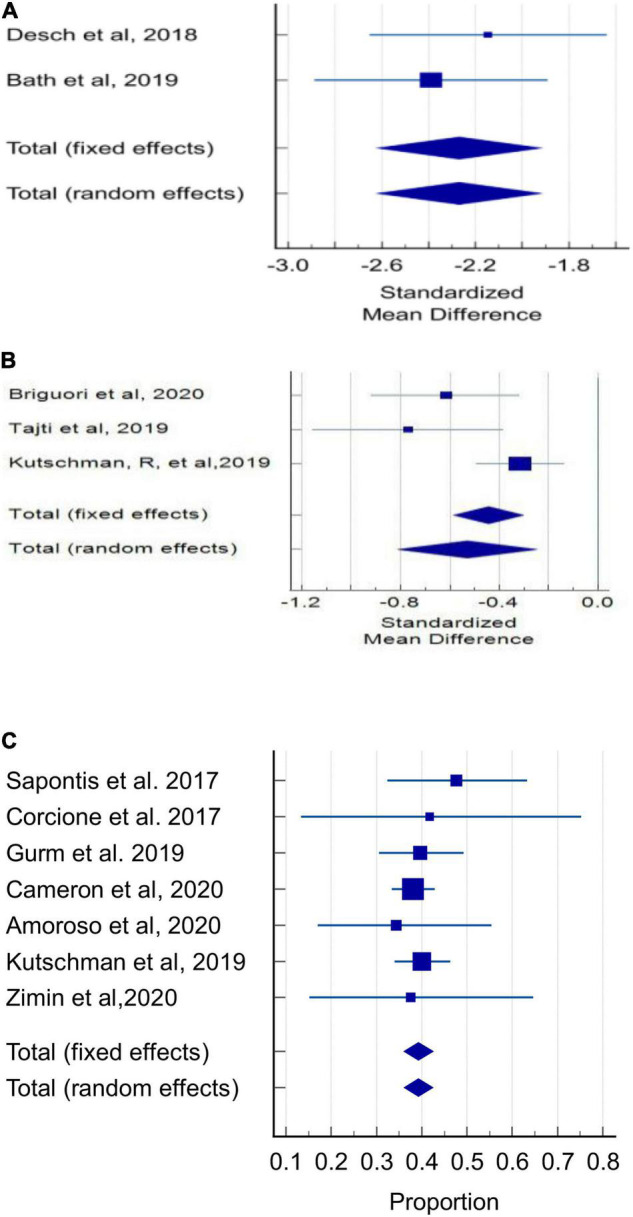
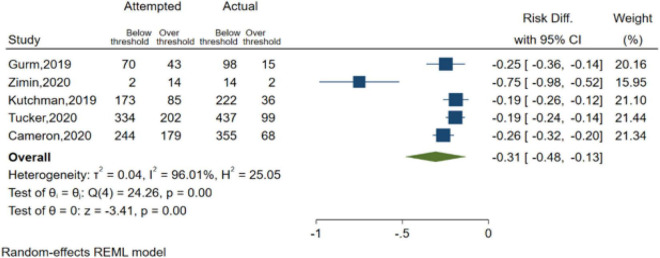
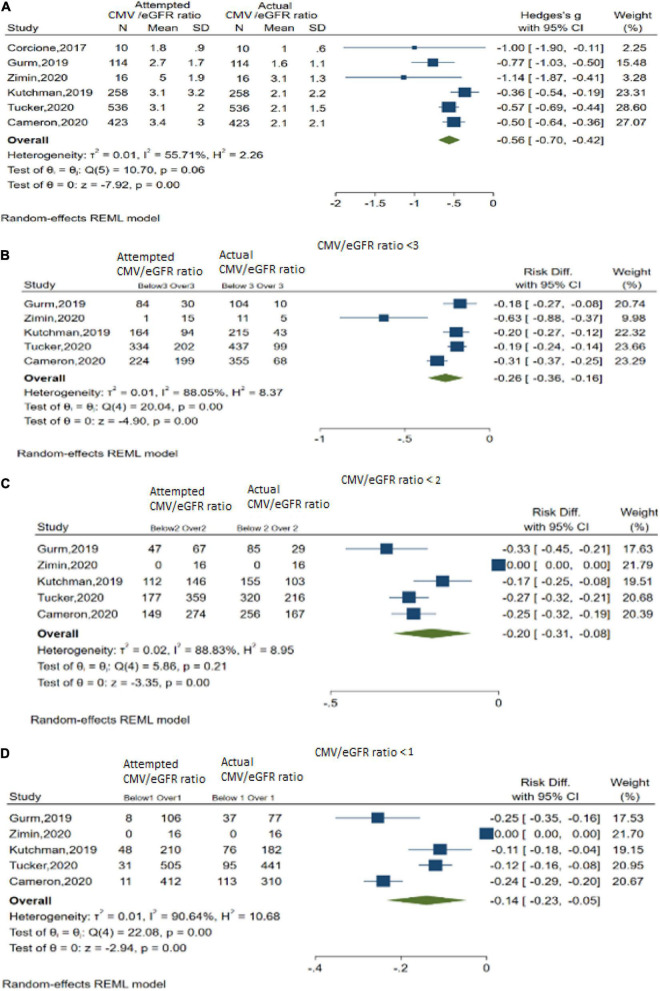
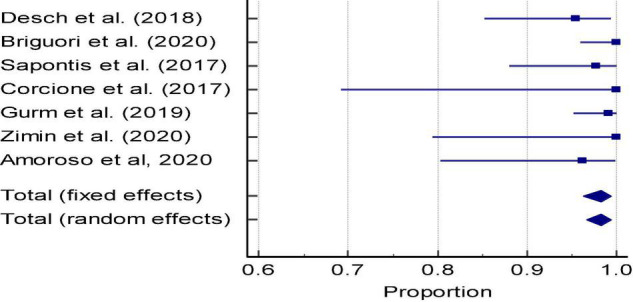
Results: The review included 17 eligible studies involving 1,731 DyeVert System cases and 1,387 control cases (without the use of DyeVert). Meta-analyses demonstrated use of the DyeVert System reduced CMV delivered to the patient by 39.27% (95% CI, 36.10-42.48%, P < 0.001), reduced CMV/baseline renal function ratios (Hedges's g, -0.56; 95% CI, -0.70 to -0.42, P < 0.001) and percentage of cases exceeding the maximum CMV threshold (risk difference -0.31, 95% CI, -0.48 to -0.13, P < 0.001) while maintaining adequate image quality in 98% of cases. DyeVert System cases demonstrated lower CA-AKI incidence vs. controls (absolute risk reduction 5.00% (95% CI, 0.40-9.80%; P = 0.03), relative risk 0.60 (95% CI, 0.40-0.90; P = 0.01) with a pooled estimate of the number needed to treat with the DyeVert System to avoid 1 CA-AKI event of 20.
Conclusion: DyeVert System use significantly reduces CMV delivered to the patient, CMV/baseline renal function ratios, and CA-AKI incidence while maintaining image quality. Accordingly, the device may serve as an adjunctive, procedure-based strategy to prevent CA-AKI. Future multi-center studies are needed to further assess effects of minimizing CMV on endpoints such as CA-AKI prevention, incidence of adverse cardiac and renal events, and health care costs.
Keywords: DyeVert System; acute kidney injury; contrast induced nephropathy; contrast media; coronary angiography; meta-analysis; percutaneous coronary intervention; systematic review.
Copyright © 2022 Tarantini, Prasad, Rathore, Bansal, Gottfried, Rosenkranz, Briguori, Yaghoubi, Mashayekhi, Javanbakht and Moloney.
Conflict of interest statement
EM, AM, and MJ were employees of Optimax Access United Kingdom Ltd., and MY was employee of Optimax Access United Kingdom Ltd. and is now an Assistant Professor at Mercer University. AP, CB, and SB were paid consultants for Osprey Medical Corporation. AR and AP received honoraria from GE Healthcare as a consultant. RG has previously received speaker fees from Shockwave Medical Inc. Osprey Medical provided funding for the professional services of Optimax/Device Access, Wendy Mills Writing LLC, and Vita Medical LLC. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Minimizing radiographic contrast administration during coronary angiography using a novel contrast reduction system: A multicenter observational study of the DyeVert™ plus contrast reduction system.Catheter Cardiovasc Interv. 2019 Jun 1;93(7):1228-1235. doi: 10.1002/ccd.27935. Epub 2018 Nov 4. Catheter Cardiovasc Interv. 2019. PMID: 30393942
-
Contrast media volume reduction with the DyeVertTM system to prevent acute kidney injury in stable patients undergoing coronary procedures.Catheter Cardiovasc Interv. 2023 Oct;102(4):655-662. doi: 10.1002/ccd.30809. Epub 2023 Sep 5. Catheter Cardiovasc Interv. 2023. PMID: 37668067
-
A Feasibility Study of the DyeVert™ Plus Contrast Reduction System to Reduce Contrast Media Volumes in Percutaneous Coronary Procedures Using Optical Coherence Tomography.Cardiovasc Revasc Med. 2021 Sep;30:40-46. doi: 10.1016/j.carrev.2020.09.040. Epub 2020 Oct 3. Cardiovasc Revasc Med. 2021. PMID: 33046416
-
Remote Ischemic Conditioning for Preventing Contrast-Induced Acute Kidney Injury in Patients Undergoing Percutaneous Coronary Interventions/Coronary Angiography: A Meta-Analysis of Randomized Controlled Trials.J Cardiovasc Pharmacol Ther. 2016 Jan;21(1):53-63. doi: 10.1177/1074248415590197. Epub 2015 Jun 24. J Cardiovasc Pharmacol Ther. 2016. PMID: 26112028 Review.
-
Radial vs femoral access for the prevention of acute kidney injury (AKI) after coronary angiography or intervention: A systematic review and meta-analysis.Catheter Cardiovasc Interv. 2018 Dec 1;92(7):E518-E526. doi: 10.1002/ccd.27903. Epub 2018 Sep 23. Catheter Cardiovasc Interv. 2018. PMID: 30244540
Cited by
-
[Effectiveness of the DyeVert Power XT system during percutaneous coronary interventions].REC Interv Cardiol. 2023 Dec 19;6(1):25-32. doi: 10.24875/RECIC.M23000411. eCollection 2024 Jan-Mar. REC Interv Cardiol. 2023. PMID: 40417724 Free PMC article. Spanish.
-
Contrast-induced acute kidney injury and its contemporary prevention.Front Cardiovasc Med. 2022 Dec 6;9:1073072. doi: 10.3389/fcvm.2022.1073072. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36561776 Free PMC article. Review.
-
Exploring software navigation tools for liver tumour angiography: a scoping review.J Med Radiat Sci. 2024 Jun;71(2):261-268. doi: 10.1002/jmrs.760. Epub 2024 Feb 2. J Med Radiat Sci. 2024. PMID: 38305074 Free PMC article.
References
-
- Tsai TT, Patel UD, Chang TI, Kennedy KF, Masoudi FA, Matheny ME, et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: insights from the NCDR cath-PCI registry. JACC Cardiovasc Interv. (2014) 7:1–9. 10.1016/j.jcin.2013.06.016 - DOI - PMC - PubMed
-
- Brown JR, Rezaee ME, Nichols EL, Marshall EJ, Siew ED, Matheny ME. Incidence and in-hospital mortality of acute kidney injury (AKI) and dialysis-requiring AKI (AKI-D) after cardiac catheterization in the national inpatient sample. J Am Heart Assoc. (2016) 5:e002739. 10.1161/JAHA.115.002739 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources