

Unicameral Bone Cysts: Review of Etiopathogenesis and Current Concepts in Diagnosis and Management
- PMID: 35547341
- PMCID: PMC9043174
- DOI: 10.1007/s43465-022-00607-6
Unicameral Bone Cysts: Review of Etiopathogenesis and Current Concepts in Diagnosis and Management
Abstract
Objective: This article aims to review the epidemiology, etio-pathogenesis and updates in clinical diagnostics and management of unicameral bone cysts (UBC).
Methods: A computerized literature search using Cochrane database of systematic reviews, EMBASE and PubMed was performed. MeSH (Medical Subject Headings) terms used in searches included the following sub-headings: "unicameral bone cyst", "epidemiology", "etiology", "pathogenesis", "diagnosis", "management" and "surgery". Studies were analyzed based on clinical relevance for the practicing orthopedic surgeon.
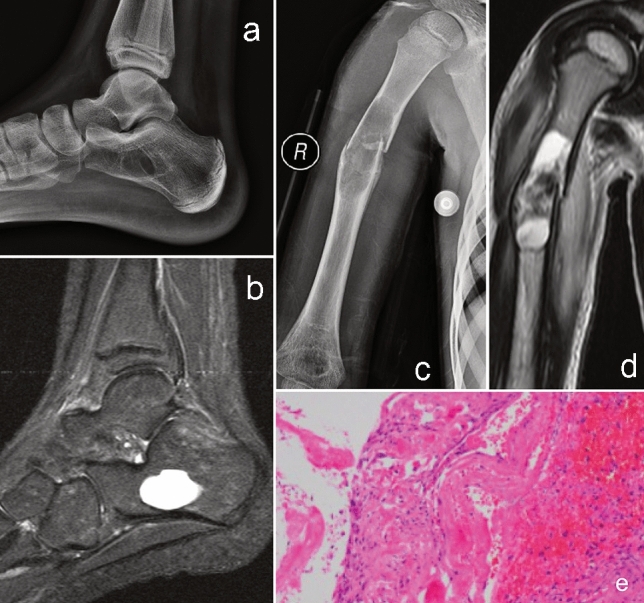
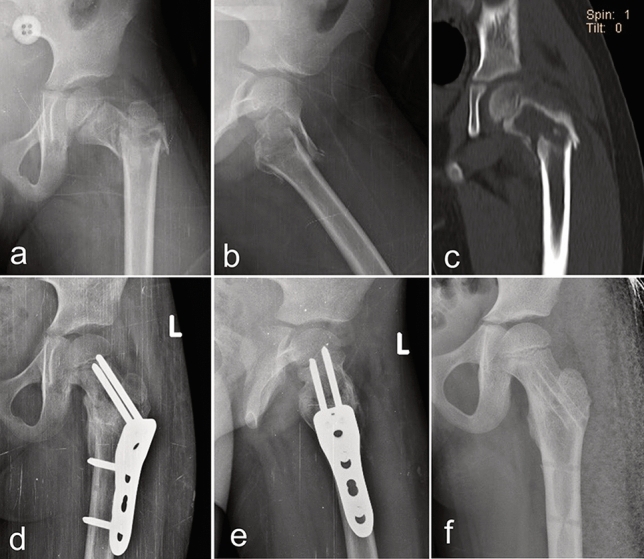
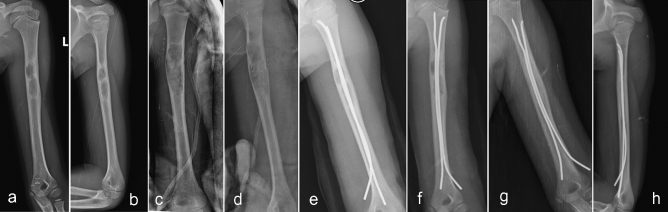
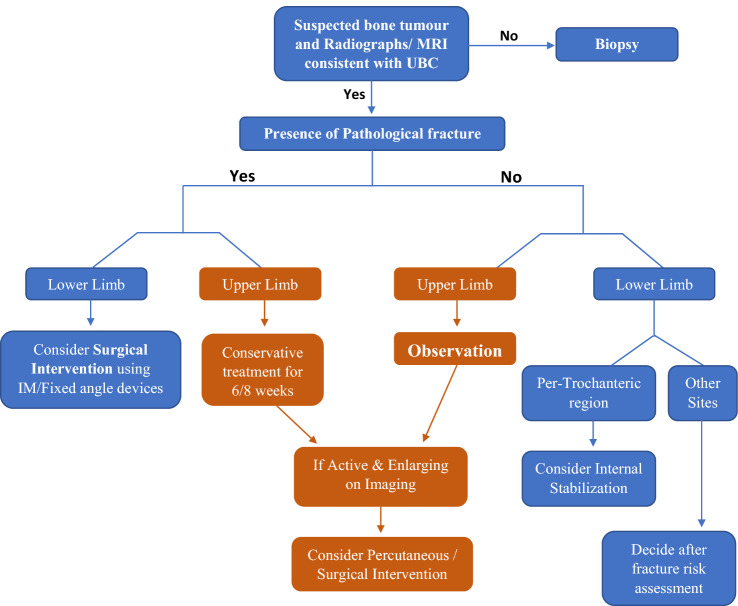
Results: UBC accounts for 3% of all bone tumors and is asymptomatic in most cases. Nearly 85% of cases occur in children and adolescents, with more than 90% involving the proximal humerus and proximal femur. Despite multiple theories proposed, the exact etiology is still unclear. Diagnosis is straightforward, with radiographs and MRI aiding in it. While non-surgical treatment is recommended in most cases, in those warranting surgery, combined minimal-invasive techniques involving decompression of cyst and stabilization have gained importance in recent times.
Conclusion: There is variation in the diagnosis and treatment of UBCs among surgeons. Due to the vast heterogeneity of reported studies, no one method is the ideal standard of care. As most UBCs tend to resolve by skeletal maturity, clinicians need to balance the likelihood of successful treatment with morbidity associated with procedures and the risks of developing a pathological fracture.
Study design: Review Article.
Keywords: Current concepts; Cyst decompression; DBM; Diagnosis; MRI; Management; Steroids; Unicameral bone cyst.
© Indian Orthopaedics Association 2022.
Conflict of interest statement
Conflict of InterestThe authors declare that they have no conflict of interest.
Figures


References
-
- Virchow R. Uber die bilding von knochencysten. S-B Akad Wiss; 1876. On the formation of bony cysts; pp. 369–381.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials