

Synchronous Parathyroid Carcinoma and Noninvasive Follicular Thyroid Neoplasm With Papillary-Like Nuclear Features
- PMID: 35547459
- PMCID: PMC9088708
- DOI: 10.7759/cureus.24006
Synchronous Parathyroid Carcinoma and Noninvasive Follicular Thyroid Neoplasm With Papillary-Like Nuclear Features
Abstract
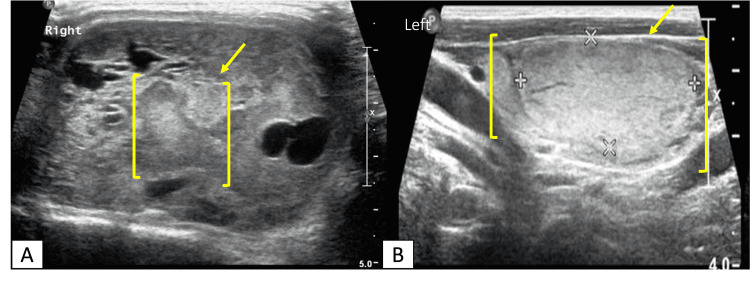
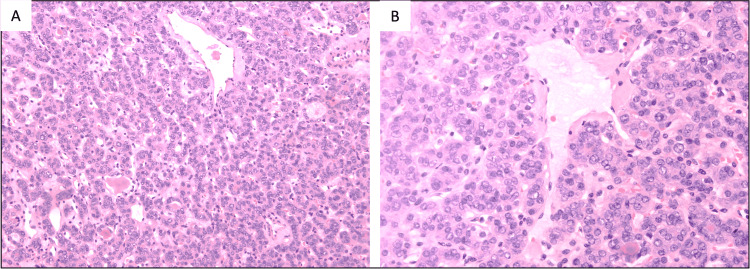
Parathyroid carcinoma is a rare cause of primary hyperparathyroidism. Compared to parathyroid adenoma, parathyroid cancer is more likely to be associated with marked levels of serum parathyroid hormone (PTH) and hypercalcemia with severe clinical manifestations. Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) is a rare variant of papillary thyroid cancer. Here, we report the case of a middle-aged woman who presented with multiple fractures and neck swelling. Neck ultrasound and fine-needle aspiration cytology revealed a provisional diagnosis of thyroid carcinoma. Parathyroid and bone scan were performed because of primary hyperparathyroidism and hypercalcemia and established the diagnosis of hyperfunctioning right-sided parathyroid tumor. Right parathyroidectomy and total thyroidectomy were performed, and the histopathological report confirmed the diagnosis of parathyroid carcinoma and NIFTP. The synchronic coexistence between parathyroid cancer and thyroid neoplasms is an extremely rare condition that prompted us to report this case.
Keywords: niftp; parathyroid carcinoma; primary hyperparathyroidism; thyroid carcinoma; total thyroidectomy.
Copyright © 2022, Alajaimi et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Parathyroid cancer: an update. Rodrigo JP, Hernandez-Prera JC, Randolph GW, et al. Cancer Treat Rev. 2020;86:102012. - PubMed
-
- Parathyroid carcinoma: challenges in diagnosis and treatment. Mohebati A, Shaha A, Shah J. Hematol Oncol Clin North Am. 2012;26:1221–1238. - PubMed
-
- Parathyroid carcinoma: clinical and pathologic features in 43 patients. Wynne AG, van Heerden J, Carney JA, Fitzpatrick LA. http://pubmed.ncbi.nlm.nih.gov/1518393/ Medicine (Baltimore) 1992;71:197–205. - PubMed
-
- Impact of reclassifying noninvasive follicular variant of papillary thyroid carcinoma on the risk of malignancy in The Bethesda System for Reporting Thyroid Cytopathology. Faquin WC, Wong LQ, Afrogheh AH, et al. Cancer Cytopathol. 2016;124:181–187. - PubMed
Publication types
LinkOut - more resources
Full Text Sources