

Pulmonary Function and Long-Term Respiratory Symptoms in Children and Adolescents After COVID-19
- PMID: 35547532
- PMCID: PMC9081758
- DOI: 10.3389/fped.2022.851008
Pulmonary Function and Long-Term Respiratory Symptoms in Children and Adolescents After COVID-19
Abstract
Background: Persistent respiratory symptoms after severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in adults are frequent, and there can be long-term impairment of pulmonary function. To date, only preliminary evidence is available on persistent respiratory sequelae of SARS-CoV-2 in children and adolescents. Our objective was to examine the long-term effects of symptomatic and asymptomatic SARS-CoV-2 infections on pulmonary function in this age group in a single-center, controlled, prospective study.
Methods: Participants with serological or polymerase chain reaction-based evidence of SARS-CoV-2 infection were recruited from a population-based study of seroconversion rates. Multiple-breath washout (MBW), body plethysmography, and diffusion capacity testing were performed for children and adolescents. Participants were interviewed about their symptoms during the acute phase of infection and long-lasting symptoms. Cases were compared with SARS-CoV-2 seronegative controls from the same population-based study with and without history of respiratory infection within 6 months prior to assessment. Primary endpoints were differences in pulmonary function, including diffusion capacity and MBW, between participants with and without evidence of SARS-CoV-2 infection. Secondary endpoints included correlation between lung function and long-lasting symptoms as well as disease severity.
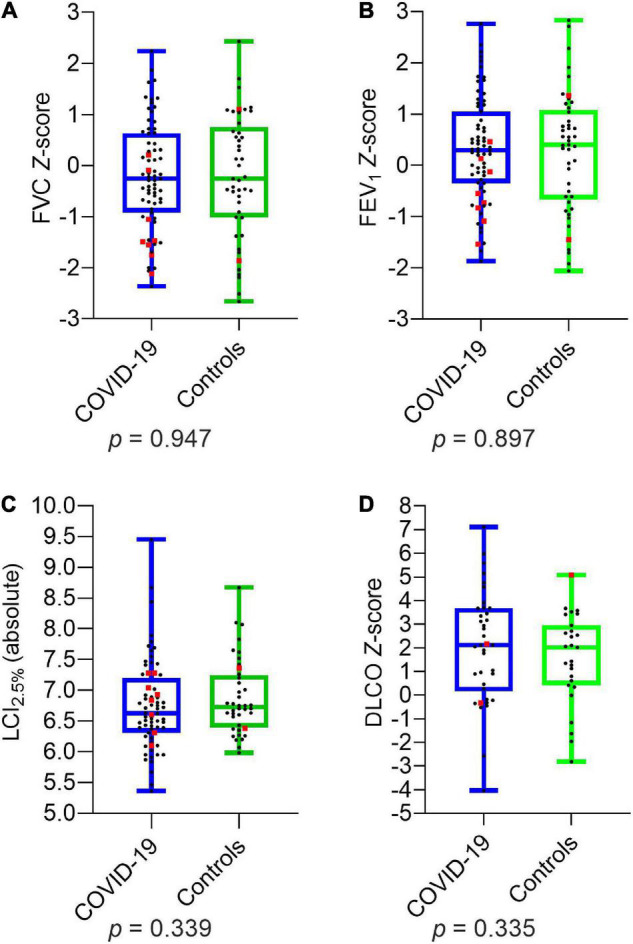
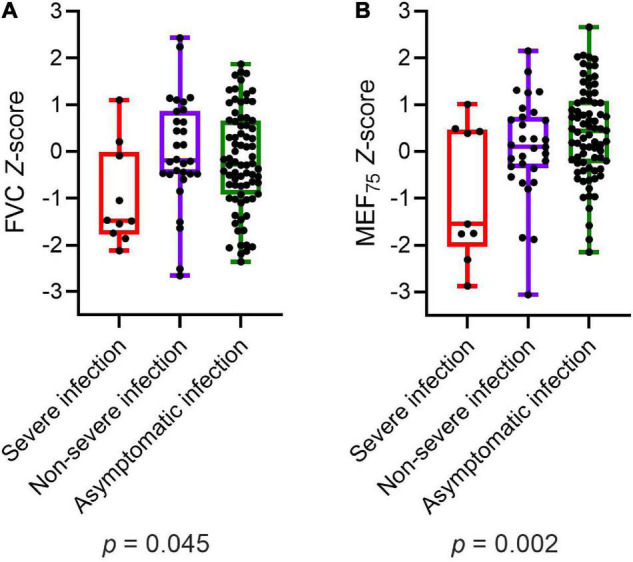
Findings: In total, 73 seropositive children and adolescents (5-18 years) were recruited after an average of 2.6 months (range 0.4-6.0) following SARS-CoV-2 infection. Among 19 patients (27.1%) who complained of persistent or newly emerged symptoms since SARS-CoV-2, 8 (11.4%) reported respiratory symptoms. No significant differences were detected in frequency of abnormal pulmonary function when comparing cases with 45 controls, including 14 (31.1%) with a history of previous infection (SARS-CoV-2: 12, 16.4%; controls: 12, 27.7%; odds ratio 0.54, 95% confidence interval 0.22-1.34). Only two patients with persistent respiratory symptoms showed abnormal pulmonary function. Multivariate analysis revealed reduced forced vital capacity (p = 0.012) in patients with severe SARS-CoV-2 infection.
Interpretation: Pulmonary function is rarely impaired in children and adolescents after SARS-CoV-2 infection, except from those with severe infection, and did not differ between SARS-CoV-2 and other previous infections, suggesting that SARS-CoV-2 is not more likely to cause pulmonary sequelae than other infections. The discrepancy between persisting respiratory symptoms and normal pulmonary function suggests a different underlying pathology such as dysfunctional breathing.
Keywords: COVID-19; LCI; SARS-CoV-2; adolescents; children; dyspnea; pulmonary function.
Copyright © 2022 Knoke, Schlegtendal, Maier, Eitner, Lücke and Brinkmann.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- National Institute for Health and Care Excellence [NICE]. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. London: National Institute for Health and Care Excellence; (2020). - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous