

Macrophages in Atheromatous Plaque Developmental Stages
- PMID: 35548412
- PMCID: PMC9081876
- DOI: 10.3389/fcvm.2022.865367
Macrophages in Atheromatous Plaque Developmental Stages
Abstract
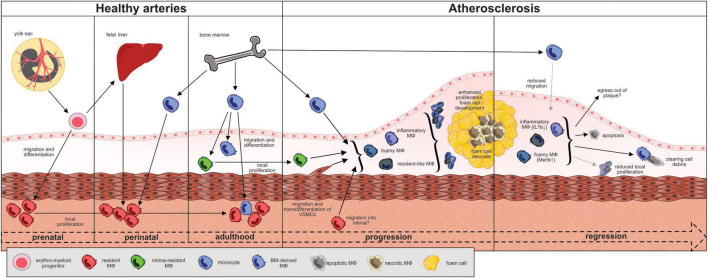
Atherosclerosis is the main pathomechanism leading to cardiovascular diseases such as myocardial infarction or stroke. There is consensus that atherosclerosis is not only a metabolic disorder but rather a chronic inflammatory disease influenced by various immune cells of the innate and adaptive immune system. Macrophages constitute the largest population of inflammatory cells in atherosclerotic lesions. They play a critical role in all stages of atherogenesis. The heterogenous macrophage population can be subdivided on the basis of their origins into resident, yolk sac and fetal liver monocyte-derived macrophages and postnatal monocyte-derived, recruited macrophages. Recent transcriptomic analyses revealed that the major macrophage populations in atherosclerosis include resident, inflammatory and foamy macrophages, representing a more functional classification. The aim of this review is to provide an overview of the trafficking, fate, and functional aspects of the different macrophage populations in the "life cycle" of an atheromatous plaque. Understanding the chronic inflammatory state in atherosclerotic lesions is an important basis for developing new therapeutic approaches to abolish lesion growth and promote plaque regression in addition to general cholesterol lowering.
Keywords: atherosclerosis; fate; macrophage; monocyte; regression; trafficking.
Copyright © 2022 von Ehr, Bode and Hilgendorf.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Regulation of Macrophage Activation and Differentiation in Atherosclerosis.J Lipid Atheroscler. 2021 Sep;10(3):251-267. doi: 10.12997/jla.2021.10.3.251. Epub 2021 Apr 28. J Lipid Atheroscler. 2021. PMID: 34621697 Free PMC article. Review.
-
Reactive oxygen species and thiol redox signaling in the macrophage biology of atherosclerosis.Antioxid Redox Signal. 2012 Dec 15;17(12):1785-95. doi: 10.1089/ars.2012.4638. Epub 2012 Jun 11. Antioxid Redox Signal. 2012. PMID: 22540532 Free PMC article. Review.
-
Vascular Macrophages in Atherosclerosis.J Immunol Res. 2019 Dec 1;2019:4354786. doi: 10.1155/2019/4354786. eCollection 2019. J Immunol Res. 2019. PMID: 31886303 Free PMC article. Review.
-
Roles of Macrophages in Atherogenesis.Front Pharmacol. 2021 Nov 26;12:785220. doi: 10.3389/fphar.2021.785220. eCollection 2021. Front Pharmacol. 2021. PMID: 34899348 Free PMC article. Review.
-
Trafficking of Mononuclear Phagocytes in Healthy Arteries and Atherosclerosis.Front Immunol. 2021 Oct 25;12:718432. doi: 10.3389/fimmu.2021.718432. eCollection 2021. Front Immunol. 2021. PMID: 34759917 Free PMC article. Review.
Cited by
-
Crosstalk between lipid metabolism and macrophages in atherosclerosis: therapeutic potential of natural products.Front Cardiovasc Med. 2025 Mar 3;12:1529924. doi: 10.3389/fcvm.2025.1529924. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40099271 Free PMC article. Review.
-
Peripheral Inflammatory Factors and Acute Myocardial Infarction Risk: A Mendelian Randomization Study.Glob Heart. 2023 Oct 6;18(1):55. doi: 10.5334/gh.1269. eCollection 2023. Glob Heart. 2023. PMID: 37811136 Free PMC article.
-
E3 ubiquitin ligase RNF128 promotes Lys63-linked polyubiquitination on SRB1 in macrophages and aggravates atherosclerosis.Nat Commun. 2025 Mar 4;16(1):2185. doi: 10.1038/s41467-025-57404-6. Nat Commun. 2025. PMID: 40038329 Free PMC article.
-
Associations between Various Inflammatory Markers and Carotid Findings in a Voluntary Asymptomatic Population Sample.Int J Mol Sci. 2024 Sep 6;25(17):9656. doi: 10.3390/ijms25179656. Int J Mol Sci. 2024. PMID: 39273602 Free PMC article.
-
Advances in treatment strategies based on scavenging reactive oxygen species of nanoparticles for atherosclerosis.J Nanobiotechnology. 2023 Aug 17;21(1):271. doi: 10.1186/s12951-023-02058-z. J Nanobiotechnology. 2023. PMID: 37592345 Free PMC article. Review.
References
-
- Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1736–88. 10.1016/S0140-6736(18)32203-7 - DOI - PMC - PubMed
-
- Saederup N, Chan L, Lira SA, Charo IF. Fractalkine deficiency markedly reduces macrophage accumulation and atherosclerotic lesion formation in CCR2-/- mice: evidence for independent chemokine functions in atherogenesis. Circulation. (2008) 117:1642–8. 10.1161/CIRCULATIONAHA.107.743872 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources